MRDA o. M.R.S.A. Anhang
[Jacqueline Smith]
A Review of Outbreaks of Necrotising Fasciitis
and indications for Homoeopathic Medicines
Objectives
To
discuss risk factors which predispose some individuals to a lowered immune system
who are therefore more susceptible to developing or contracting Necrotising
Fasciitis (= N.F.)
To
examine details of documented and possible bacteria involved in the process of
suppuration leading to necrosis.
To
consider relevant homoeopathic philosophy in relation to susceptibility,
maintaining causes, and predisposition.
To
outline the disease process involved which may lead in some individuals, to
developing N.F.
To
present a resume of individualised homoeopathic remedies potentially suitable
for use in all stages of the disease process outlined in Objective Four.
Background
In June 2000, 22 drug users in Scotland and 21
between Dublin and Manchester, died after contracting (or developing)
Necrotising Fasciitis, and again in July 2001 eight individuals were affected,
either fatally or requiring surgical debridement +/o. partial amputation. These
cases were thought to be the result of using contaminated heroin for injecting
in cases of drug addiction. The condition itself is described as “. .. a
rapidly progressive soft-tissue infection that involves superficial and deep
fascia leading to thrombosis of cutaneous vessels and
gangrene of underlying tissues.” It was first documented by Fournier in 1883,
and Meleney isolated a particular bacteria as a
causative factor in 1924. The term ‘necrotising fasciitis’ was ascribed to
Wilson, who, in 1952, noted that an “essential component” of gangrene with a
specific bacteria, involved the deep fascia. The condition can occur in any
anatomical location, usually at a distance from any trauma but also at affected
sites. Other names: Fournier’s Gangrene (genital), Meleney’s
Ulcer or Hospital Gangrene etc., often indicate either anatomical sites or
places where infection was contracted or developed. Conventional therapy
involves antimicrobial treatment with e.g. Penicillin, aminoglycoside,
metronidazole etc. and Hyperbaric Oxygen Therapy
(HBO) and surgical excision (debridement and amputation when considered
necessary).
Risk Factors
[Jacqueline Smith]
Several factors conventionally regarded as
leading to possible susceptibility in contracting or developing N.F. The
greatest of these is that of having a ‘compromised’ immune system, which is
noted in conditions such as (Diabetes Mellitus/malignancy/renal
impairment/trauma). In this discussion intent on reviewing the specific factors
in relation to the circumstances of intravenous drug users who may be homeless,
2 of the above noted conditions are worthy of further exploration. In the first
instance, similar to Diabetes Mellitus II, where a state of ketosis may develop
due to the inability of the body to utilise carbohydrates and glucose, it is
worth pointing out that it is also possible for ketosis to develop in states of
starvation or eating disorders. The result being, that fats and proteins become
the primary energy sources, which may produce ketones
in the blood, and thereby lead to ketoacidosis. In
the report of a survey carried out in 1999 by the Office of National Statistics
titled, ‘Health and Well Being of Homeless People in Glasgow’, June 2000, “19%
of respondents had eaten only once in the day prior to interview and 5% had not
consumed any food at all. 15% of respondents did not consume any hot food
(excl. drinks) in the day prior to interview.”
It would seem probable that in such
circumstances, it would be possible for heroin addicts who are also of homeless
status to be at similar risk to developing a condition akin to ketoacidosis, which may also result in renal damage. In
addition, it is well known that nutritional deficiencies play a decisive role
in the prevalence and severity of microbial diseases in under privileged
people. The rate of wound healing is also markedly influenced by dietary
factors [deficiencies of some vitamins (Vitamins C, E, K, B6) and Minerals
(Calcium and Iron)].
The citing of ‘trauma’, as a further risk
factor is particularly apt in the present examination of the incidence of N.F.
in intravenous drug users. ‘Trauma’, here being defined as: “…any injury caused
by a mechanical or physical agent.”
Heroin addiction most often requires the use of
intravenous means whereby the subjects repeatedly inject the drug, causing
puncture wounds, often several times daily for, perhaps, a duration of some
years, with little or any use of disinfecting measures. Thus creating a higher
than usual risk of infection at multiple sites, most often on arms and legs but
the groin area is also used amongst others, as more accessible veins become
unusable.
In the outbreaks of N.F. documented here, this
is all the more relevant, for it has been discovered that all the cases had a
significant factor, i.e. the injection has been made directly into muscle
tissue or accidentally into other tissues when a vein has been missed. This
assertion also brings to bear the immune inhibiting effects of drugs themselves
as a risk factor to infection which include non-steroidal inflammatory
preparations such as aspirin, ibuprofen, naproxen etc. that inhibit the
inflammatory mechanism that makes tissue repair possible. Steroid use is
particularly implicated, possibly due to the fact that cortisone interferes
with the production of antibodies under certain conditions. This immunologic
inhibition cannot account entirely for the infection enhancing effect. In
addition to interfering with antibody production, cortisone influences many
other physiologic processes, some of which may affect directly or indirectly
the response of the body to infection. Interference with the inflammatory
response and with the activity of the reticulo-endothelial
system, disturbance of the intermediary metabolism, and activation of proteo-lyctic enzymes are but a few of the effects of
cortisone that might be important in this regard.
The habitual use of heroin, (= diacetyl-morphine, a semi- synthetic compound derived from
morphine and stronger than the natural drug), which has its effects principally
on the Central Nervous System (CNS) and also affects some peripheral organs
such as the alimentary tract and the respiratory system, is a definite factor
in compromising the immune system. Morphine usually neither eliminates the
psychological perception of pain nor blocks the sensation. Although there are
exceptions, the person knows that pain continues, but he or she is not
disturbed by it. The associated fear and tension subside so that the pain
becomes bearable. These reactions signify the effects on the CNS but the
opiates may also change the activity of peripheral nerves that conduct messages
to and from the brain. The enkephalins involved are
found in neurons in the spinal cord and portions of the hind and mid-brain
which transmit pain and related sensory signals (for example, heat and cold),
and in parts of the mid-brain associated with movement, mood and behaviour.
The enkephalins are
also found outside the central nervous system in the neurons of the periphery
and the gut. These effects have relevance in two areas in connection with this
investigation: the fact that the addict despite feeling hunger is able to
ignore these feelings. This can result in the production of acids in the gut
which having no food to breakdown will tend to become destructive to the
alimentary tract itself. The other danger is that by being able to ignore
sensations of heat, pain and even fear for health, any inflammation, abscess
formation or numbness can continue unabated.
Bacteriological Factors
In the past, several types of bacteria have
been identified as being involved in the presentation of N.F. On this basis,
two types of N.F. had been labelled, i.e.
a)
Polymicrobial,
involving a number of organisms in various combinations
b)
Pure group A Streptococcal said to be haemolytic,
(rupture of RBC membrane). In direct relation to the cited outbreaks, Clostridiun Novyi Type A among
others, was isolated from 18 of the people who developed N.F. in June 2000. Some
of these bacteria are known as being indigenous (= present in a healthy state)
to the human body, e.g. Bacteroides, Staphylocci, Streptococci, Pseudomonas aeruginosa,
Clostridium etc.
Two aspects are known to be observable
concerning these micro-biota:
That most micro-organisms commonly harboured by
the body in a state of health are capable of exerting a wide range of
pathological effects under special conditions and,
Many of the micro-organisms classified as pathogens,
indeed probably all of them, often persist in vivo without causing overt
disease.
As has been previously noted, nutritional
deficiencies, exposure to toxic agents, and certain kinds of physiological
stress are among the many causes of disturbances associated with disease
processes caused by indigenous microbiota. In other
words, some form of pathological or at least abnormal state must exist before
indigenous bacteria can multiply to such an extent that it causes deleterious
effects.
George Bernard Shaw: Pasteur suggested that a
physiological disturbance might in certain cases be the primary cause of the
infectious process rather than its consequence, when he said:
“The characteristic microbe of a disease might
be a symptom instead of a cause.” Early in the investigations of 2000, Dr
Laurence Gruer, Consultant to the Greater Glasgow
Health Board commented that:
“It is quite possible that no single cause for
the illnesses will be identified. Many injectors in the affected areas of
Glasgow have said that their recent supply of heroin has required unusually
large amounts of citric acid to be added before it can be dissolved for
injecting. A variety of different bacteria normally found on the skin have been
isolated from tissue or blood from several patients. It is likely that
injection of the unusually strong heroin and acid mixture can cause severe
damage to muscle and other tissue. This may then create the conditions for
harmless bacteria present in heroin or carried on the needle from the skin to cause
serious infection.”
Clostridium Novyi,
Type A, was isolated in some, though not all, recent or current cases of N.F.
at the time and described as an “…’anaerobic’ [= they only grow in the absence
of oxygen (= dead tissue)].
Some Clostridium can not only cause severe
infection in damaged tissue but can also produce very powerful toxins. They can
also exist in for years in dust or soil as dormant spores, only becoming
activated when the conditions are right.” But it was only previously been known
to cause serious infection in domestic animals; very rarely in humans and is
commonly found in soil and animal faeces. Other types of Clostridium have been
located in intestinal flora of the human where it is non-spore forming.
It is therefore a matter of postulating whether
the Clostridium isolated in the cases cited, is the actual cause originating in
contaminated heroin supplies and therefore exogenous. In classical infections
of exogenous origin, the determining etiological event of the disease is said
to be exposure to the infective micro-organism. This was yet to be made clear
in the present situation. The author has been unable to locate documentation on
this particular strain of Clostridium (ie. Novyi) in standard textbooks on microbiology and this raises
two questions:
In which conditions, if any, has it been
previously been isolated?
Or, is it a possible new mutation arising from
this particular combination of factors met in this incidence of drug injectors?
In indigenous microbial disease, the immediate
cause is the environmental factors that upset the biological equilibrium
normally existing between the host and the microbial agents. The documented
factors common to many (but not all) of the affected were:
They
are all Heroin Injectors, whose supply source may or may not have been the
same.
Many,
if not all, used more Citric Acid than usual to dissolve the drug for
injection.
The
subjects all injected into muscle or tissue other than a vein.
If the source of supplied heroin was the same
and all users of this supply increased the quantity of Citric Acid - plus the
involvement of the injection into muscle and other connective tissue, (not
particularly uncommon in heroin addicts), not all heroin injectors likely to
have used this batch of the drug under these circumstances, have succumbed to
either infection or development of N.F.
It would have to be considered somewhat as a
result of this combination of factors or it would suggest another unidentified
predisposing factor.
Dr. Jai Lingappa,
Epidemic Investigation Officer at the Centers for
Disease Control in Atlanta, commented that:
“A lot more work still needs to be done to
clarify how exactly the Clostridium Novyi is
contributing to the illness……..We also want to learn more about why these
people became sick and others didn’t.”
The purpose of reviewing this serious
condition, (N.F), with the prospective use of Homoeopathic medicines for
treatment in mind, is to put forward an approach that will to a degree bring
into congruence the determinants of infection and the determinants of disease
and present a means of treating the pathological processes which can ensue from
both exogenous and indigenous causes, and to understand and control the
processes responsible for converting so-called infection into overt disease.
This approach is found in Homoeopathic philosophy and practiced in the
homoeopathic treatment of both individuals and genus epidemicus.
Relevant theory is summarised in the next section.
Even from the viewpoint of conventional
medicine, a person in robust health may easily resist exposure to even the most
virulent microorganisms. The degree of resistance can change from hour to hour
and day to day depending upon exhaustion, starvation, cold, overwork, emotional
stress, etc. It has been stated clearly in a standard textbook on microbiology
used in all universities and medical schools in the U.S., that the
susceptibility factor is so significant that it is virtually impossible to
decide the infective dose of a specific microorganism. (24) In the cited cases
of those developing N.F., this study has identified at least some of the major
factors related to increased susceptibility to developing a seriously life
threatening infectious disease and this is further explained in Homoeopathic
philosophy by considering not just the ‘compromised’ immune system but by also
considering the effects on the Defence Mechanism of the human organism. This
defence mechanism is known in homeopathy as the Vital Force and is considered
in terms of electro-dynamic vibrations, which involves a great degree of
complexity.
“The vital force level of the human organism is
considered the dynamic plane, affecting all levels of the being at once with
varying degrees of harmony and strength. It is a highly complex, fluid,
flexible, and energetic process, simultaneously responding to and affecting the
surrounding environment……The whole organism, and any component of it, can be
strengthened or weakened depending upon the degree of harmony, resonance, and
force of the morbific or therapeutic influence
applied to it.”
When the strength of a noxious trigger is
stronger than the strength of the vital force, the defence mechanism is called
into play to counteract the stimulus. If the vital force is so weakened by
exciting and maintaining causes, any powerful noxious trigger would alter the
state of the entire organism without adequate defence, and death would rapidly
ensue. There is a latent period before actual symptoms develop, during which
the defence mechanism begins to adjust to the effect of the stimulus. In
bacterial infections this ranges from hours to days.
From this premise it should be clear that
disease is a result of a morbific stimulus which
resonates with the particular susceptibility of the organism. This stimulus is
known as the exciting cause and may be a microorganism, a foreign chemical, an
emotional shock, a vaccination, etc.
Maintaining causes are those factors external
to the organism which, because they continue to affect the individual over a
period of time, maintain the individual in a weakened state eg.
Lack of nutrition, unsanitary or damp living conditions, drug addiction;
conventional drugs prescribed for long periods or repeated often in short
periods of time (also regarded as Iatrogenic miasms),
repeated emotional trauma, in short, many of the factors previously
mentioned. But yet, the predisposition
underlying much of these areas of susceptibility is the Fundamental Cause.
Useful to the physician in assisting him to
cure, are the particulars of the most probable exciting cause of the acute
disease, as also (are) the most significant points in the whole history of the
chronic disease to enable him to discover its fundamental cause, which is
generally due to a chronic miasm. In these
investigations, the ascertainable physical constitution of the patient, his
moral and intellectual character, his occupation, mode of living and habits,
his social and domestic relations, his age,… etc., are to be taken into consideration.”
(Par. 5, The Organon of Medicine, Samuel Hahnemann,
5th & 6th Edition, B. Jain Pub. Reprint 1992)
The theory of Chronic Miasms
is complex and involved and it is not within the scope of this review to give a
full explanation of such. In summary, it is sufficient to say that a miasm is a resulting stereotypical disease condition,
sometimes heredotransmissable, which can be latent or
active, acute or chronic. Nevertheless, it is always the result of both a
maintaining cause (hence the lingering disposition) and an exopathic
exciting cause (the noxious trigger).
There is one miasmatic
pattern, relevant to this review that has been recognised for most of
Homoeopathy’s history ie., the Luetic
Miasm. This particular pattern is in essence one of
destruction and disintegration. There will often be a predilection in the
family history to similar patterns of destructive illnesses, eg. Syphilis, alcoholism, conditions where ulceration has
taken place or a tendency to necrosis, etc. When active and predominant in an
individual, this pattern will taint and distort expression at all levels,
mental, emotional and physical. In the individuals involved in the outbreaks of
N.F. cited , the destructive pattern is essentially seen in addictive habits
concerning the use of heroin and often several other substances. There exists a
craving for acidic or spicy foods in general, there is a metabolic tendency to
acidity and they are often of a temperament conducive to states of rage; that
is when not suppressed by drugs. The effects of this pattern whereby heroin
addiction is a symptom result in destruction not only of the immune system and
particular bodily organs and systems e.g. the heart and circulatory system, but
as noted, affects the intellectual faculties, the emotional responses and
subsequent behaviour destroys family and social contact.
With regard to the ‘contagious principle’,
Hahnemann, (1755-1843, founder of Homoeopathy), though not having the benefit
of a microscope, put forward an uncannily accurate explanation more than half a
century ahead of Robert Koch and others. He suggested in 1832 (Lesser Writings,
p.758) that cholera, for instance, was caused by “…an enormous …brood of
excessively minute, living creatures.”
He also regarded each epidemic (acute miasm) as having features of its own (the genus epidemicus) And since it is always the product of a single
cause it will, in all individual cases, be amenable to one and the same
specific remedy, the epidemic’s simillimum.
The Disease Process
In this section, the disease process taken into
account is that which begins, for our purposes, from the available information
on the circumstances and states of individuals who were involved in cited
presentations of actual or threatening N.F.
They are individuals who are:
Intravenous Drug users i.e., heroin injectors;
Experience a chaotic lifestyle, which often includes bouts of
homelessness.
Deaths
predominantly in females.
In the first assertion, two factors are
particularly important:
1a). Lowered Immune System due to chronic
heroin use (poisoning);
1b). Bodily subjected to repeated trauma from
puncture wounds.
In the second assertion, two factors are again
considered of import:
2a). Immune system
further compromised by chaotic lifestyle (times of homelessness), resulting in:
Reduced intake of adequate food and nutrition.
Exposure to the elements.
2b). Less access to
medical services when required, unless in an emergency.
This information provides some clues to the
degree of susceptibility at the general level of health and the particular
susceptibility at the physical sites by repeated trauma and risk of infection.
Schematic Evolution of Possible Disease
Processes in General Terms
Comp.
I. S. –> Repeated Puncture Wounds –> Abscess
Formation –> Necrosis of tissue at local sites with
possibility of developing N.F.
Comp.
I.S. –> Vein injection infected by
exogenous pathogen –> Septicaemia –> Possible development of N.F.
Comp.
I.S. –> Injection into Fascia,
infected by exogenous pathogen and/or high levels of acid at site creating
environment for mutation of indigenous bacteria. –> Rapid development of N.F.
Schematic Evolution of Disease Processes
through Particular Levels and Systems
This section is based on available information
from previous documentation and current GGHB Bulletins.
Symptoms Levels
physical Levels Process
Pyrexia Circulatory System Genetische Inflammation
Response
Discoloration
(local) Cutting blood vessels Inflammation
local
Pain
Suppuration Peripheral Nerves/Epidermis Sensation/Dysfunction
Numbness Peripheral Nerves Sensation/Dysfunction
Thrombosis Subcutan
Veins & Arteries Dysfunction/Structural Change
Gangrene
(Fascia) Adipose Tissue Destruction of Fascia (Superficial
& Deep)
Connection
Tissue of Muscle
Secondaire Necrosis Stomach/Heart/Artery Walls Desintergration of Systems & Organs
The following section is adapted from ‘Thorsons Encyclopaedic Dictionary of Homoeopathy’ by Harald Gaier. (Pgs. 130-132, Pub.
Thorsons,1991) due to its admirable scientific clarity.
“DISEASE and DRUG ACTION in HOMOEOPATHIC
CONGRUITY”
Applied therapeutic science requires a
coincident parallelism between the symptom complexes of both the disease and
the drug of choice on as many of the first seven under-mentioned points of
comparison as possible. Obvious incongruity in any comparative aspect
frequently amounts to symptom dissimilarity in the case, allowing for the
elimination of many otherwise eligible remedies, facilitating the process of repertorisation.
1.
Generic Similarity
Homoeopathicity of type
of affliction; describes the identity in the class of affections induced by
both the natural disease of the patient and the experimental disease of the
drug to be used: eg.
a) if the illness is febrile, the remedy must
be pyro-genetic;
b) if the disease is an inflammation, the drug
of choice will be an irritant, etc.
Causal
Similarity
Homoeopathicity of
formative affectors; means that the antecedent
concomitants present when the disease arises will substantially narrow the
field of contenders among drugs to be used:
eg.
neuralgia induced by injury to a nerve is different from one brought on by
shingles and that again is also distinct from one that comes on with gout.
Parallels in Symptom Modalities
Homoeopathicity of
modalities. Meteorological and thermal influences, cosmic rhythms, mental
factors, physical conditions (including movements and rest), relation to food
and drink, location, laterality and time are circumstances that can contribute
to making symptoms
a) better
b) worse,
c) appear
d) change.
Symptom Character Resemblance
Homoeopathicity in the
quality of abnormal sensations. All sensations have a distinct character: for
instance, a gnawing pain, a burning pain, a tearing pain etc. are distinctly
different from each other.
The character of such sensations are to be
alike in both the disease and the drug action.
Constitutional
Compatibility
This describes the aggregate of patients’
common features. It is used to identify patients according to their
temperament, appearance, certain characteristics of behaviour and their
variance from the normal, which should be compatible with the corresponding
remedy.
Synchronicity of Symptom Evolution
Homoeopathicity of pharmocodynamic devolution; meaning that various
developmental aspects of the disease process of the patient must synchronise
with the developmental pathogenicity inherent in the
drug to be applied.
Concordance of Emotional Symptoms
Homoeopathicity of
disposition; matching emotional and/ or the intellectual symptoms. Since mental
and emotional symptoms are in evidence well ahead of functional and
morphological changes when disease develops, they frequently provide very early
indications for homoeopathic treatment.
Matching of Three or More Guiding Symptoms
Multiples of semiological
homoeopathicity. Reliance on the coincidence of
three, but preferably more, striking symptoms, evident in both the artificial
illness of a drug as well as in the phenomena of a disease, rests on the
mathematical law of permutations. If three distinctive symptoms of a case can
be found to have been experimentally produced by a medicine, there is already
considerable likelihood of its acting on the same parts and in the same manner.
Ranking
Many homoeopaths are guided by Robert Gibson
Miller, who in 1910 proposed ranking the above points of comparison in the
following order of priority:
matching mental & emotional symptoms;
correspondence between modalities of time, season, motion, locality,
sensation etc.
similarity of pronounced cravings and aversions;
menstrual, or hormone-related, changes in state in both the natural and
the artificial diseases;
resemblance between the particulars as well as the generals of both
diseases, where only the peculiar, unexpected, striking or unaccountable
symptoms are of significance;
common
symptoms, as featured in standard non-homoeopathic disease classifications.
The Simillimum is the
medicine, which in its manifestations most clearly reflects the total symptom
picture of the individual’s diseased state, which will certainly cure that
patient, if the patient’s condition is within reversible limits. In relation to
the symptoms available from the documentation in the author’s possession, which
have little or no individuality, it is less likely that the most accurate simillimum will be found.
But as will be explained, it is not always the
best remedy to prescribe even if it were possible (by taking information from
those who are displaying symptoms associated with the recent outbreak or who
are thought to be at greatest risk.)
Contra-indication Against Administering Simillimum
In a patient, whose disease is terminal and
which may be in its final stages, namely where the life force is hopelessly
overwhelmed by the forces of disease, or in many emergencies, it is absolutely
contra-indicated to prescribe the individual’s simillimum,
which would, in these circumstances, only be able to produce an aggravation
hastening death. In such an instance functiotropic, organotropic or pathotropic
remedies ought to be the homoeopathic drugs of choice, with the intention of
inducing a measure of improvement for the limited period remaining to the
patient.(29 Therefore, the remedies identified by using predominantly common,
general and particular symptoms which have no modalities, will be sufficient
when given at the appropriate phase in the disease process and may reflect more
the nature of the Genus Epidemicus rather than the simillimum of the individual patient.
Finding the Genus
Epidemicus.x
Although, it is not as yet possible to find, or
would in some cases be inappropriate to utilise the simillimum,
many of the above mentioned principles will still be employed to find the
remedy or remedies that come closest to the picture of the genus epidemicus. This means that, depending on at which stage of
the disease process the remedy is administered, there is a possibility of
preventing the development of N.F. or reducing the effects of infection before
it reaches a life threatening degree. Symptoms will be taken from all general
and particular disease processes outlined above:
remedies for various stages of the disease.
Wounds: 1. Penetrating (Punctured) +.Stab
wounds, Synth.Pg.1720; APIS. Arn. Carb-v.
Cic. Hep. HYPER. lach. LED.
Nit-ac. sil. sulph.
2. Bluish + Black. Synth.
Pg.1719; Apis. China. LACH.
3. Suppurating. Synth.
Pg 1720; Arn. asaf. Bell.
Calc. Calen. Cham.Chin. Hep
Lach. Led. Merc. Sil. Sulph
4. Dissecting. Synth.
Pg.1719; Anthraci. Apis. Ars. kreos. Lach.
Led. Pyrog.
5. Gangrene of. Synth.
Pg.1719; Anthraci. ARS. Bell. Calen.
Carb-v. China. LACH. sil.vip.
Inflammation: 6. Wounds. Synth.
Pg.1619; Arn. hyper. lach.
led. sulph.
7. Gangrenous. Synth.
Pg.1618; ARS. bapt. Carb-v.
hep. Iod. kreos. LACH. merc. Phos .SIL
Abscesses: 8. To abort. Synth.Pg.1547: Apis. arn. bell. bry. calc. calc-s. hep. merc.
Absorption of pus, Synth.Pg.1547: Iod; LACH; Phos; Sil.
10. Gangrenous: Ars;
asaf; carb-v; chin; hep; kreos; LACH; merc; nit-ac; phos; sil.
Fever
Septic:
Synth. Pg. 1487: ANTHRACI. Apis.
ARN. ARS. BAPT. Bell. BRY. Carb-v. LACH. Merc. PHOS. PYROG. SULPH.
Zymotic: Synth.Pg.1490: Anthraci.
apis. ARN. ARS. BAPT. Bell. BRY. carb-v.
hyos. ip. LACH. Merc. op. Phos. Puls. Pyrog. Sulph.
Mind:
13. Morphinism: Synth. Pg.152; Ars. bell. calc; cham; hyos. ip.
lach. merc. op; phos; puls.
Each remedy is rated by the number of rubrics
in which it appears and by how prominent or characteristic it is in the remedy
picture, ie. Those in CAPITALS, are given 3 points;
Those in Italics, are given 2 points; and those in plain type are given 1
point.
REMEDIES (present in SIX or more Rubrics) +
Points Rating / No. of Rubrics
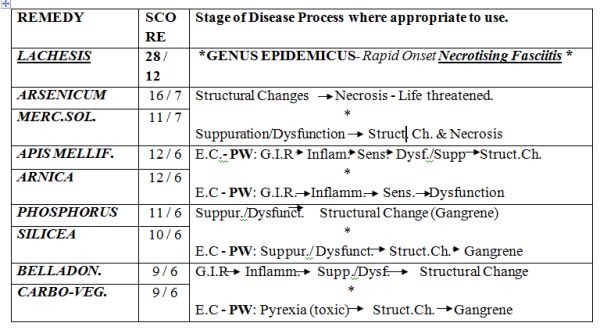
KEY: E.C. = Exciting Cause
PW: = Puncture Wounds G.I.R. = General
Inflammatory Response
Necrotising Fasciitis
+ Genus medicus
Lach.x
Source: This remedy is prepared from the venom
of the viper, Lachesis trigonephalus,
the Surucuccu or Bushmaster snake of South America.
The venom is preserved dry or in glycerine.
Poisoning Symptoms: All the vipers are
venomous; severe pain comes on at the site of a bite, bloody serous discharge
and ecchymoses in the vicinity of the bite and
thrombosis, followed, if not at once fatal,
by local inflammation and sloughing, and even
gangrene.
Swelling and black or purple discolouration may
follow. Fever, with delirium and blood poisoning, sets in, followed by
suppuration, haemorrhage or gangrene. Death may follow a bite from the
following causes:
If a
vein has been pierced, quickly follows thrombosis;
after
some hours from heart failure, through paralysis of the vasomotor centres;
after a
few days from secondary bleeding;
later
from septic infection of the necrotic area around the bite.
Pharmacology: The venom of Lachesis
contains a full range of potent enzymes, proteolytic,
cytolytic, neurotoxic and coagulant.
One or more of these effects may predominate. The blood is attacked primarily,
1.
nervous system aroused and excited,
2.
The main affinities are with the blood, causing
disintegration of red cells, lowered coagulability
after initial tendency to thrombosis, and impaired resistance to infection with
associated liability to gangrene and necrosis.
3. Also
the CNS, with ensuing delirium, coma and paralysis of vital centres. Also with
the cardiovascular system as evidenced by hypotension, cold sweats and
collapse.
Therapeutics: The great blood-disintegrating
(haemolytic) powers of Lachesis are utilized in a
number of febrile, septic, toxic and typhus-like conditions, present in many
diseases, and in some forms called ‘malignant’ exanthems,
where the body resistance has more or less completely broken down. When this
point is attained the distinguishing or diagnostic features of the particular
diseases have largely disappeared.
As Professor Teale,
in a lecture before the British Homoeopathic Society, explained: “Widely
different bacteria may produce very similar clinical features… when profound
poisoning occurs, instead of the poisoning becoming more, it becomes less
characteristic, and clinically is seen to be in the typhoid state.”
Leading Indications:
Severe cases where “blood-poisoning” is marked:
‘low’ fevers, where blood-destruction or haemolysis is conspicuous, conditions
called typhus-like (typhoid), or septic after parturition or autopsy wounds.
Such conditions occur late in many fevers.
Milder cases, where vascular erethism is conspicuous-palpitation, hot flushes,
sleeplessness. Such a state is frequent at the menopause or after arrest of
physiological discharges or the sudden arrest
of pathological discharges, and relieved by the
restoration of them. Shock may cause such a state.
Though
sensitive to either extremes of temperature, chiefly noted for intolerance of
hot weather, hot rooms, etc. (direct rays of the sun).
Local
symptoms are frequently left-sided or move from left to right.
Sleep
is not easily wooed; when it comes it is restless and wakes < in every
respect, so that he fears to go to sleep.
The
mental state varies… Incoherence, degenerating to muttering delirium in fevers,
is characteristic.
Over-sensitiveness to surface contact (touch), and to constrictions, or
even to clothing which is not too tight (neck, abdomen, etc.)
A
bluish hue around wounds, ulcers, etc. from blood pigment, or venous stasis.
Difficulty of swallowing, especially fluids, regurgitation through the
nostrils.
Onset
of discharges tends to relieve most symptoms.
Craving
for alcohol, even in teetotallers.
Bleeding in many parts, blood dark and thin; ecchymoses.
Thin,
melancholy, indolent person, changed physically and temperamentally by illness.0
<: morning/after sleep/spring &
summer/extremes of temperature/constriction/contact/acids/alcohol/empty
swallowing/hot drinks/motion/stooping or lying/emotions/lying on l. side
(palpitation);
>: Onset of discharges.
Causation: Injuries. Punctured wounds. Poisoned
wounds. Vexation. Anger. Jealousy. Alcohol. Sun.
Materia Medica for Remedies at Similar or Earlier Stages of
Necrotising Fasciitis
The following remedies will be given in less
detail than above but will show greater characteristic features for the
purposes of differential diagnosis in other stages of the disease process which
may or may not result in development of N.F.
Ars.x
Therapeutics:
Ars.: a
universally acting substance, attacking, as it does, nearly every organ and
tissue of the body, that it is necessary to be acquainted with the general
characteristics that will reveal it as the simillimum.
Tendency to rapidly proceed to a condition of malignancy, ie., diseases assume a grave form, to the destruction of
tissue, to a general lowering of the vital forces, and haemolysis, ending, if
not checked, in death.
Another
characteristic is prostration, a prostration that is out of proportion to the severity
of the complaint. The patient is exhausted after the slightest exertion.
Nevertheless, they are extremely restless. Restless with the pains, must
walk about, which helps. Also mental restlessness, feels impelled to move and
when too prostrate wants others to move them from bed to
bed or
room to room.
Pains
have a burning character where-ever situated in the body and there is often a
sensation of hot fluid coursing through the veins.
Generally chilly, despite the burning pains.
Periodicity is a feature of Arsenicum. It
occurs every other day, every fourth, seventh, or fourteenth day: the more
chronic the complaint the longer the cycle.
Putridity of discharges. This is an accompaniment of its ulcerations
whether internal or external, and of the tendency of its ulcerations to go on
to necrosis and its inflammations to become gangrenous.
Allied
with this is inflamed and ulcerated parts bleed readily. Haemorrhages occur
from the lungs, bowels, kidneys and uterus.
<: midnight and after/3 h./cold/lying with
head low/exertion/after (cold) food and drink.
>: from warmth, movement;
Merc.x
Source: a) Also known as Mercurius
Oxydulatus Niger from its black colour, was the
ammonium nitrate salt of mercury introduced by Hahnemann into medicine in 1788.
2 (NH2Hg2)NO3H2O.
It was prepared by precipitating Mercury from
its solution in nitric acid by means of caustic ammonia. Trituration.
Mercurius Vivus. Hg. Hydrargyrum. Argentum vivum. Metallic Mercury. Quicksilver.
Although H. proved Merc.,
he recommended the use of triturations of the pure
metal in practice as being the simplest mercurial preparation, and more easily
obtained and equally available with Merc. for
prescribing on the symptoms of the latter. Trituration.
Therapeutics:
A feature of Mercurius
is very easy exhaustion after quite slight exertion. There is a tendency to
emaciation and paretic weakness, associated liability to fainting attacks or
sudden myocardial failure.
Blood dyscrasias
occur, resulting in profound anaemia which renders the subject liable to ready
suppuration, characterised by sanious pus or necrotic
ulceration.
Leading Indications.
Cachexia, anaemia, exhaustion, emaciation.
Salivation; stomatitis.
Increase and alteration of secretions, which become thin and excoriate.
Ulceration of skin and mucous membranes.
Perspirations which do not relieve and are foul-smelling.
Thirst,
with moisture of mouth and tongue.
<
night/from warmth of the bed.
Moist
eczema and intertrigo.
Nocturnal bone pains.
Low-grade suppurations, which are acrid and blood-stained.
Tremors
of course character that tend to become convulsive.
Green,
bloody or mucous stools with tenesmus, “a cannot get
done feeling.”
Foul
body smell.
Mercurial
symptoms occurring in syphilis.
Catarrhs of mucous membranes, with increased mucous.
<: at night/both heat & cold/warmth of
bed/draughts/bending forwards/after eating/lying on right
side/touch/pressure/motion/exertion/sweet food/lamp-/firelight;
>: rest/weeping/coitus;
Apis.x
Source: The honey bee is the source of this
remedy, the whole insect being used in the preparation of the mother tincture
or dilutions of the poison with alcohol.
Pharmacology: The chemical composition of the
bee venom remains obscure, although various fractions, such as histamine, hyaluronidase and a bradykinin
have been identified. It is said to
be a toxalbumin, and
its effects are similar to those of other animal poisons, such as the toxalbumins of the snakes, spiders, lizards, etc. Bee venom
is known to have haemolytic, haemorrhagic
and neurotoxic
effects in addition to its profound histamine activity.
In addition to haemolysis, coagulation of
fibrinogen and increased permeability of capillaries, there is also a lowering
of surface tension and membranes potential, resulting in reduction of osmotic
pressure and facilitates diffusion of fluids, leading to oedema and effusion.
Leading Indications:
Aggravation from heat in any form.
Over-sensitiveness: of skin, of mind, of organs.
Sadness, indifference, suspicion, jealousy.
Foolish
or childish behaviour.
Stinging, burning pains, with rapid change of site.
Violence and rapidity of complaints.
Right-sided; symptoms go from right to left.
Absence
of thirst where it is expected, ie., during heat, and
also generally.
Tight,
constrictive sensations: in throat, larynx, chest, abdomen.
Inflammation and oedema: of skin, mucous membranes, serous membranes,
synovial membranes, subcutaneous tissues.
Urticaria and erysipelas.
Cerebral affections, especially in children; meningitis, cri cerebral.
Morning
diarrhoea.
Prostration; faintness.
<: 15 h.
(chills)/morning/evening/night/(radiant) heat/close rooms/touch/pressure/lying
down/getting wet;
>: cold
(washing)/expectoration/sitting/changing position;
Arn.x
Therapeutics: It is especially suited to case when
any injury, however remote seems to have caused the present trouble. After
traumatic injuries, overuse of any organ, strains. Arnica is disposed to
cerebral congestion. It acts best in plethora, in debilitation with
impoverished blood, cardiac dropsy with dyspnoea. A muscular tonic. Traumatism
of grief, or remorse. Influenza. Limbs and body ache as if beaten; joints as if
sprained. Bed feels too hard. Sore, lame, bruised feeling.
Marked effect on the blood. Affects the venous
system inducing stasis. Thrombosis. Haematocele. Ecchymoses
and haemorrhages. Relaxed blood vessels, black and blue spots. Tendency to
haemorrhage and low-fever states. Tendency to tissue degeneration, septic
conditions, abscesses that do not mature.
If the malady advances more definite stupor
develops, and though when roused the patient begins to answer a question
correctly, he lapses in the middle of a sentence into muttering delirium or
unconsciousness. When a patient has arrived at this mental state he is well on
in a typhus, enteric, malignant malaria, yellow fever, or sepsis (surgical, peurperal or other). The concomitants in the shape of
muttering delirium, fever, rapid, weak pulse, dusky skin, possibly with ecchymoses, or congestive patches, dry tongue, sordes etc. some or all of these will now be present. (42).
Prophylactic of pus infection. (Shroyens, Synthesis,
Edit.5.2., Pg. 1790)
<: Movement (walking/going
upstairs)/movement/spinal pain/wrist pain/pain < inspiration;
>: Movement. (Sore feeling from lying on one
part, but the relief is only temporary);
Phos.x
Source: The homoeopathic preparations were made
from phosphorus obtained from bone ash. This was the yellow toxic variety,
which may also be obtained from the mineral apatite, from animal bones and
from basic slag, a by-product of steel-making.
Potencies are prepared from a saturated solution of the yellow phosphorus in
alcohol.
Therapeutics: In typhoid-like conditions
Phosphorus is recognisable by:
Abdomen distension; sore, very sensitive to
touch. Stools offensive, bloody, involuntary. The anus appears to remain open.
<: lying on left side, >: right. Burning in stomach: burning thirst for
cold water.
Desire for ice cream.
Fear: alone/in dark/of thunder; Suspicious;
Sil.x
Therapeutics: Skin: Lymphatic swellings and
abscesses, even with fistulous ulcers.-Engorgement, induration
and suppuration of glands.-Abscesses which do not break, but burrow under the
skin; exanthemata in general which corrode and spread. Ulcers in general;
wherever pus is discharged from any part of the body; ulcers burning, scabby;
indolent; when circumscribed with redness; very high, hard ulcers; with proud
flesh; with corroding pus; smell very offensive. Inflammation, softening(swelling),
and ulceration of bones. Mild and malignant suppurations, esp. in membranous
parts. Small wounds heal with difficulty, and suppurate profusely. Mental and
Emotional: weak, nervous, easily irritated, faint-hearted; yielding, giving up
disposition, “grit all gone.”
<: From cold or draft/motion/open air/at new
moon;
>: In a warm room/wrapping up head/magnetism
and electricity;
Bell.x
Therapeutics:
Leading Indications
Congestions and inflammations of a violent and intense character.
Pains
and symptoms come and go suddenly and are violent.
Tendency to delirium of an active and violent kind: hallucinations,
fears of imaginary things (“a black dog”) with desire to escape.
Tendency
to twitchings, jerkings and
convulsions.
Burning
fever and rapid pulse, which is strong and bounding; early stages of
inflammations.
Dryness
and heat of the skin and mucous membranes.
Hypersensitivity to all impressions, drafts, noises, pressure etc.
Great
thirst not relieved by drinking.
< in
the afternoon (15 h.) and till after midnight.
Predominance of affections on the r. side.
Symptoms < in the horizontal position (head).
Tendency to rapid formation of pus in external inflammations.
Carb-v.x
Source: Vegetable charcoal. It is generally
made from poplar, beech or birch wood, and raised to the third potency by trituration.
Pathogenesis: Charcoal has the property of
absorbing gases in its interstices, and thus ordinarily contains quantities of
oxygen which, when the charcoal is brought into contact with decomposing
organic matter, is released, and oxidises the
putrefying mass, while at the same time the charcoal adsorbs the gases that are
formed by the oxidising process. It has no direct action on the microbes
of putrefaction, but favours the development of
the aerobic organism at the expense of the anaerobic.
Leading Indications:
Desire
to be fanned rapidly in stomach and respiratory complaints.
Burning
internally, cold externally; burning characterizes many of the Carbo-v.
Surface
cold; dusky blue nails; dilated capillaries and veins, cold sweat. Numbness of
parts lain on.
Haemorrhages, passive oozing of dark thin blood.
States
of collapse, surgical shock.
Septic
conditions, putrid discharges.
Conditions where there is a lack of reaction.
Low
states of vitality with venous engorgement.
Fever:
tertian type, beginning 9 - 10 h. Thirst in cold stage, none in hot.
<: morning on waking/evening/hot, damp
air/warmth/brandy and wine/butter/pork/rich food/abuse of quinine and mercury;
>: eructations/warm
covering/being fanned;
Potency
Is defined as: “The especially produced
capability in a medicine to effect a dynamic stimulus in the appropriate
patient (and)… is the stage of remedial activity to which a drug has been taken
by means of a measured process of deconcentration, with succussion,
or by trituration, of the medicinal substance, which
is thus brought to a state of diminutive or infinitesimal subdivision.”
Extensive investigative studies of recorded pathogenetic experiments were carried out by Henri Voisin to assess the time passed before particular
reactions happened in provers and also to
confirm what had already been established by
clinical usage. His results were that, in general:
Low
potencies are best suited to organic disease;
Medium
potencies are most effective for influencing function;
High
potencies produce the best response in mental & emotional symptoms.
For our purposes in this review, it is
sufficient to assert that it has become accepted practice that lower potencies
are often given in repeated doses when prescribing on the basis of morbid
anatomy
(as recommended by Richard Hughes, 1836-1902),
and in some acute diseases provided there is no irreversible tissue
destruction. But it should also be remembered that a remedy, if well indicated
in terms of the law of similars,
would be homoeopathic even without recourse to a potency thereof, as exemplified
by the occasional use of mother tinctures, whenever one of these happens to be
the most appropriate form of the remedy for the
particular case.
Discussion
Based on the information reviewed concerning
both the accepted theory and practice of treatment of the disease process,
which can result in states of inflammation, suppuration, gangrene or necrosis
as a consequence of puncture wounds (caused by
drug injection/other injections), repeated over time or infected by an
exogenous pathogen in those with a compromised immune system (C.I.S.), and
with theory and practice in homoeopathy for
treatment of similar states with similar causes, it would seem more than
plausible to conclude that homoeopathic treatment is a viable alternative when
antibiotics are proving ineffective, as has
been the case in some instances, when N.F is rapidly developing, or as a
complement to such treatment as debridement and surgery when required, (Carb-v.
in relation to Hyperbaric Oxygen Therapy).
Treatment using homoeopathic medicines is also
highly effective in earlier stages of the disease process, which may help
prevent the potential development of suppuration or sepsis at either local
sites
or its more serious effects when toxins have
entered the bloodstream. The author has considered some of the reasons, which
contribute to a lowered state of immunity. Homoeopathic philosophy has
also been included, which provides an added
perspective to the subject of predisposition in this particular disease
manifestation, by identifying an innate pattern, which may be found to provide
clues
as to why these particular individuals
succumbed to severe infection requiring surgery or consequently died, rather
than many others in the same or similar circumstances.
Without exact figures as to the number of
people who were of homeless status amongst those affected by the cited
outbreaks, it is impossible to conclude just how influential this status would
be to
the potential rapid development of septic
states, although it is clear they would be considered to be at greater risk for
the reasons outlined above. Nevertheless, the author feels this is an important
question for both the self-care of intravenous
drug users who are also homeless but also for health-care and housing
providers. Furthermore, the aim of this review has been realised, in that, six
main
remedies have been identified as being
appropriate for treatment of the afore-mentioned stages of this disease process
from inflammation through to necrosis and a resume of these medicines has
been provided with additional notes regarding
appropriate choice of potency if prescription of same should be considered.
ZEIT ONLINE
Gesundheit
Eine Hoffnung namens Pathoblocker
[Lydia Klöckner]
Gerda Jäker begriff nicht, warum die
Pflegerin plötzlich einen Mundschutz hatte. Auch die grüne Plastikhaube, die
Gummihandschuhe und den Einwegkittel hatte die junge Frau vorhin noch nicht
getragen. "Das Labor hat angerufen", sagte sie nun mit ungewohnt
ernster Miene. "Die Ergebnisse sind da, Sie haben einen Keim in der Wunde,
wir müssen Sie isolieren, es ist MRSA."
Gerda Jäker erinnert sich noch gut an den
Abend Ende März, als sie diese Diagnose bekam. Denn danach änderte sich alles
für die 80-jährige Dame mit der Querschnittslähmung. Ursprünglich war sie wegen
zweier wunder Stellen am Gesäß -Folgeerscheinungen des ständigen Liegens- ins
Krankenhaus gekommen. Nun bereiteten ihr die Wunden nicht mehr nur leichte
Schmerzen, sondern Todesangst. "Ich hatte in der Zeitung allerhand Schauergeschichten
über diesen Keim gelesen", erinnert sie sich. "Ich dachte, jetzt
endet alles und ich sterbe – ich habe drei Tage nur geweint."
Jäker hat die Infektion überlebt, doch von einer Heilung ist sie noch immer
weit entfernt. Seit Wochen liegt sie in ihrem Einzelzimmer, in dem es immer
leicht nach Desinfektionsmittel riecht. "Ich fühle mich wie im
Gefängnis", sagt sie. Alles, was sie berührt, muss sofort sterilisiert
oder entsorgt werden. Jeder, der ihr Zimmer betreten möchte, muss sich zunächst
in Schutzkleidung hüllen. Selbst ihren Mann, ihre Töchter und ihre Enkel
bekommt Jäker niemals unvermummt zu Gesicht.
Probleme wie aus Vorkriegszeiten
Wann Frau Jäker wieder entlassen werden kann,
wissen die Ärzte nicht. Die Wunden müssen erst keimfrei sein. Hier liegt das
Problem: MRSA (= Methicillin-resistenter Staphylococcus aureus) lässt sich
nicht so leicht ausmerzen. Es gibt kaum noch Antibiotika, die gegen den Keim
etwas ausrichten können.
Unheilbare Infektionskrankheiten, ratlose Mediziner – das erinnert an
Vorkriegszeiten, an düstere Kapitel unserer Geschichte, als der Mensch
Bakterien hilflos ausgeliefert war. Dank Antibiotika wähnen wir uns heute auf
der erfolgreichen Seite im Kampf gegen die Keime. Doch das ist eine gewaltige
Fehleinschätzung: Eine Studie der Weltgesundheitsorganisation (WHO) ergab
jüngst, dass sich auf der ganzen Welt immer mehr resistente Keime ausbreiten,
gegen die Antibiotika nicht mehr wirken. "Eine postantibiotische
Ära, in der verbreitete Infekte und harmlose Verletzungen wieder tödlich sein
können, ist eine sehr reale Möglichkeit für das 21. Jahrhundert", warnte
die WHO. Doch Geschichten wie die von Gerda Jäker
zeigen: Das postantibiotische Zeitalter hat schon
längst begonnen. In der Europäischen Union erliegen Schätzungen zufolge
jährlich mehr als 25.000 Menschen den Folgen einer Infektion mit resistenten
Bakterien. Und bald könnten wir endgültig mit leeren Händen dastehen.
Die Bakterien werden stärker und stärker
Was tun wir ohne Antibiotika? Mit dieser Frage beschäftigen sich Menschen
auf der ganzen Welt, sie ist zu einer der entscheidenden der gesamten
Menschheit geworden. In ihren Laboren tüfteln Forscher an Alternativen zu
herkömmlichen Bakterienkillern. Ihre Ideen mal vielversprechend, mal
realitätsfern – und mal auch etwas ekelhaft. Aber sie vereint eine gemeinsame
Vision: von einer Medizin, die ohne traditionelle Antibiotika auskommt. Von
Therapien, die sogar gegen multiresistente Bakterien helfen -ohne neue
Resistenzen hervorzurufen. Dafür gehen sie ganz neue Wege. So wollen sie die
Keime zum Beispiel nicht mehr abtöten- was lange Zeit als Ideallösung galt.
Die Fähigkeit zur Resistenz ist für Bakterien eine Art Geheimwaffe.
Dabei nutzen sie eine Schwäche aus: Selbst aggressive Antibiotika töten nie
alle Keime ab, sondern nur etwa 99%. Meist überlebt eine kleine Gruppe von
Außenseitern: Man kann sie sich vorstellen als ein widerständisches gallisches
Dörfchen. Sie haben zwar keinen Zaubertrank, aber besondere genetische
Eigenschaften, die ihnen die Fähigkeit verleihen, Antibiotika abzuwehren.
Dieses übrig gebliebene, resistente Grüppchen von Bakterien erhält plötzlich
jede Menge Platz, weil das Antibiotikum ihnen die Konkurrenz vom Leibe schafft.
Das gallische Dörfchen wächst zur Millionenmetropole heran, und die Keime können
ihre Resistenzgene -die Teile ihres Erbguts, die sie
gegenüber Antibiotika unempfindlich machen- über spezielle Transportmechanismen
an benachbarte Kolonien und sogar andere Arten weitergeben. So fördern
Antibiotika nicht nur die Vermehrung resistenter Bakterien, sondern auch die
Ausbreitung der Resistenzen selbst. Wo viele Antibiotika zum Einsatz kommen,
etwa in der Tiermast und in Krankenhäusern, werden resistente Keime also
geradezu gezüchtet. Höchste Zeit, umzudenken. Wenn Antibiotika nicht mehr wirken,
brauchen wir originellere Behandlungsmethoden.
Eine davon ist eine neue Therapie gegen den Durchfallkeim Clostridium difficile. Er befällt
meist Menschen, deren natürliche Darmflora geschwächt ist, etwa durch eine
vorangegangene Antibiotikatherapie.
Mangelt es an gutartigen Bakterienstämmen, können sich schädliche Clostridien leichter ausbreiten. Hier setzt die neue
Methode an: Die Patienten erhalten "Stuhlspenden" -kleine Portionen
von Fäkalien von gesunden Verwandten, in denen sich vor allem gute Bakterien
tummeln. Sie werden in den entzündeten Darm geschleust. Geht alles gut,
etablieren sich die neuen Bakterienstämme in ihrer neuen Umgebung und machen
den Clostridien Konkurrenz.
Die Methode mag abstoßend klingen, doch die Erfolge sprechen für sich.
Die erste klinische Studie führte die Medizinerin Els
van Noord mit ihrem Team vor etwa einem Jahr an der
Universität Amsterdam durch.
Die Forscher teilten 29 an Clostridien
erkrankte Menschen nach dem Zufallsprinzip einer von zwei Gruppen zu: 16 von
ihnen erhielten Fäkalien von Verwandten, den restlichen 13 verabreichten die
Ärzte das Antibiotikum Vancomycin. Die Ergebnisse
waren so spektakulär, dass die Mediziner die Studie abbrechen mussten: Aus der
Stuhlspendengruppe erholten sich 15 der Probanden binnen weniger Tage. Vancomycin verhalf dagegen nur 4 von 13 Studienteilnehmern
aus der Kontrollgruppe zur Genesung. Die Fäkalientherapie erwies sich als so
wirksam, dass es geradezu unethisch gewesen wäre, sie den anderen Patienten zu
verwehren. Den einen Antibiotika-Ersatz wird es wohl
nicht geben
Die Aussagekraft der Studie ist begrenzt, allein wegen der niedrigen
Probandenzahl. Trotzdem ist die anfangs als "Ekeltherapie"
verspottete Heilmethode heute so anerkannt, dass immer mehr Kliniken sie
durchführen. Es könnte sie künftig sogar als Pille geben: Kanadische Forscher
haben spezielle Gelatinekapseln entwickelt, mit denen die Fäkalbakterien in den
Darm geschleust werden können. Leider sind die Anwendungsgebiete begrenzt. Das
Prinzip, böse Keime mit guten zu verdrängen, kann zwar durchaus auch gegen
andere Krankheiten helfen -Wundentzündungen zum Beispiel-, aber eben nicht
gegen alle.
"Die eine neue Wundermedizin, die Antibiotika ein für alle Mal
ablöst, wird es wohl nie geben", sagt Winfried Kern, bis 2013 Vorsitzender
der Deutschen Gesellschaft für Infektiologie und
derzeitiger Sprecher der Arbeitsgemeinschaft wissenschaftlicher
Fachgesellschaften in der Infektionsmedizin. "Aber vielleicht viele
unterschiedliche Therapieformen, mit denen man gezielter gegen die krank
machende Wirkung verschiedener Bakterien vorgehen kann." Spezifität sei das Zauberwort des postantibiotischen
Zeitalters -für jede Krankheit eine maßgeschneiderte Therapie. Dazu müsste man
die Infektionserreger und ihre Auswirkungen auf den Körper aber noch besser
kennenlernen. Wie genau machen sie uns krank? Warum schaden sie uns? Je besser
man das weiß, desto gezielter kann man sie unschädlich machen – sogar ohne sie
töten zu müssen. Wenn man Bakterien ihrer Waffen berauben könnte, hätte unser
Immunsystem bessere Chancen, mit ihnen fertigzuwerden.
Bisher zielten Therapien aber vor allem darauf ab, sie möglichst schnell und
großflächig auszumerzen.
Neuere Ansätze richten sich nicht gegen die Erreger selbst, sondern vor
allem gegen ihre schädlichen Eigenschaften. Hinter diesem Prinzip steckt eine
ganz neue Denkweise: Die krank machenden Prozesse, die sie in unserem Körper
lostreten, rücken nun ins Blickfeld, und es werden Wirkstoffe entwickelt, die
diesen Prozessen entgegenwirken könnten, sogenannte Pathoblocker.
Etwa gegen Bakterien mit dem Namen Pseudomonas aeruginosa. Diese Keime schaden vor allem durch die
Absonderung eines Stoffs namens Pyocyanin, der unser
Gewebe angreift. Bei Menschen mit geschwächtem Immunsystem kann das Bakterium
Lungenentzündungen, Wundinfektionen und Blutvergiftungen hervorrufen. Die
Erreger produzieren das Gift allerdings nur als Gruppe, in der sie sich über
chemische Signale miteinander verständigen. So können sie als Gemeinschaft
agieren und mit vereinter Kraft einen Angriff starten. Um den abzuwenden,
müsste man die Kolonie also am Kommunizieren hindern. Genau das gelang kürzlich
Wissenschaftlern vom Helmholtz-Institut für Pharmazeutische Forschung im
Saarland. Sie entwickelten einen Wirkstoff, der den Bakterien quasi den
Briefkasten zuklebt, ihre Kommunikation so unterbricht und verhindert, dass sie
einen Angriff aushecken können.
Im Labor ging der Plan auf: Bakterienkolonien, denen die Forscher den
Wirkstoff verabreicht hatten, produzierten tatsächlich weniger giftiges Pyocyanin. Auch erhöhte der Klebstoff die Überlebensrate
von Larven und Würmern, die mit Pseudomonas infiziert
waren. Zwar lassen sich Erfolge aus Tierversuchen nie ohne Weiteres auf den
Menschen übertragen – schon gar nicht, wenn es sich bei den Tieren um Larven
handelt. Interessant ist der Ansatz dennoch. "Im Gegensatz zu Antibiotika
greift unser Wirkstoff nicht in lebenswichtige Stoffwechselwege der Bakterien
ein, sondern blockiert deren Pathogenität",
erklärt Rolf Hartmann vom Helmholtz-Institut. Das Mittel tötet die Bakterien
also nicht und verschafft mutierten, resistenten Keimen so auch keinen Vorteil.
Anders ein Antibiotikum: Es würde einen Großteil der Kolonie ausrotten und
dadurch den resistenten Keimen bessere Bedingungen bieten.
Auch der Biologe Rolf Kümmerli forscht mit
seiner Arbeitsgruppe an der Universität Zürich an Möglichkeiten, Infektionen zu
bekämpfen, ohne Bakterien zu töten. Sie wollen die Keime am Wachstum hindern,
indem sie sie davon abhalten, Eisen aufzunehmen. Das benötigen sie nämlich zum
Wachstum und zur Energiegewinnung. Pseudomonas aeruginosa setzen sogenannte Siderophore
– griechisch für "Eisenträger" – frei, mit denen sie sich
Eisenteilchen außerhalb der Zelle angeln und sie aufnehmen können.
Gallium legt die Bakterien lahm
Mit einem Trick gelang es den Forschern, die Siderophore
lahmzulegen: Sie verabreichten den Bakterien Gallium, ein Metall, das Eisen
ähnelt. Anstelle des Eisens nahmen die Siderophore
nun Gallium auf – was die Bakterien daran hinderte, zu wachsen. Und wenn Keime
nicht weiterwachsen, schaden sie ihrem Wirt weniger.
Zwar wirken auch einige Antibiotika auf diese Weise. Dennoch bezweifelt
Kümmerli, dass Bakterien irgendwann Resistenzen gegen
Gallium entwickeln, weil die meisten bekannten Resistenzmechanismen sich nur
gegen Wirkstoffe richten, die in die Bakterienzelle hineingelangen. Manche
Keime haben etwa spezielle Pumpen in ihrer Hülle, die Antibiotika zurück in die
Umgebung schleusen. "Wenn man Gallium richtig dosiert, gelangt es aber gar
nicht erst ins Innere der Bakterien, sondern wirkt von außen. Es kann also auch
nicht hinausgeschleust werden", so der Forscher. Die richtige Dosierung zu
finden sei allerdings nicht einfach.
Von der Marktreife ist Kümmerlis Idee noch
weit entfernt. Zudem existieren neben Pseudomonaden noch Tausende andere Keime,
die uns Menschen auf verschiedenste Art und Weise krank machen können. Brauchen
wir also wirklich gegen jeden Keim eine eigene, maßgeschneiderte
Kampfstrategie? Nicht unbedingt. Eine Gruppe von Ingenieuren hat eine Methode
entwickelt, die zumindest gegen mehrere verschiedene Infektionen helfen könnte:
Sie bastelten im Labor schwammähnliche Kügelchen aus Nanopartikeln,
die Toxine der Erreger Staphylokokken und
Streptokokken gewissermaßen aufsaugen können. Die Gifte dieser Bakterienarten
löchern die Hüllen unserer Blutzellen und zerstören sie auf diese Weise.
Genau diese Angriffstaktik machten sich die Forscher für das Design der
Nanoteilchen zunutze: Sie überzogen sie mit
Zellhüllen roter Blutkörperchen. Anschließend spritzten sie die verkleideten
Partikel in die Blutbahn von Mäusen und verabreichten ihnen dann eine tödliche
Dosis des Bakteriengiftes. Tatsächlich fielen die Giftteilchen auf den Trick
herein: Sie bohrten sich in die Hüllen der als Blutkörperchen getarnten
Kügelchen. Dank der Nanoteilchen überstanden fast 90%
der Labormäuse die letale Giftdosis. Als die Ingenieure den Mäusen die
Schwämmchen erst nach dem Toxin spritzten, überlebte immerhin noch knapp die
Hälfte. Nach 40 Stunden war im Blut der überlebenden Nager nur noch etwa die
Hälfte der Nanoschwämmchen übrig geblieben. Ihr
Körper hatte also nicht nur die Kügelchen, sondern auch die Gifte abgebaut –
offenbar ohne dabei selbst Schaden zu nehmen. "Das Besondere an dieser
Methode ist, dass sie auch multiresistente Erreger ungefährlich machen
könnte", sagt einer der Erfinder, Liangfang
Zhang. "Außerdem kann man damit ein breites Spektrum von Bakteriengiften
neutralisieren."
Gegen Erreger, die uns schon durch ihre bloße Anwesenheit schaden,
hilft diese Methode natürlich nicht. Wenn etwa Darmbakterien unsere Harnwege
und Nieren überschwemmen, verursachen sie eine schmerzhafte Entzündung –
einfach weil sie dort nicht hingehören. Um die Infektion zu heilen, muss man
die Erreger also beseitigen – aber nicht unbedingt töten: Die schwedische
Chemikerin Anette Svensson hat Stoffe entdeckt, die
die Keime der Fähigkeit berauben, sich in der Blasenschleimhaut festzusetzen.
Sie und ihre Mitarbeiter fanden heraus, dass bestimmte Stoffe Bakterien daran
hindern können, sogenannte Pili auszubilden. Das sind
haarähnliche Anhängsel, mit denen sich die Keime an Wirtszellen verankern. Wenn
sich die Erreger nicht festhalten können, werden sie mit dem Urin wieder
ausgeschwemmt. Das zeigte ein Experiment mit infizierten Mäusen.
Mit unkonventionellen Methoden gehen Forscher inzwischen gegen
Bakterien vor. Sie entwickeln neue Möglichkeiten gegen einen Feind, der immer
stärker wird. Nanoschwämmchen haben eine Oberfläche,
die der eines roten Blutkörperchens ähnelt. Daher fangen sie Bakterientoxine ab, die normalerweise die Blutkörperchen
angegriffen hätten.
Sogenannte Adhäsionshemmer verhindern, dass sich Bakterien an
menschlichem Gewebe wie dem der Blase verankern können – etwa indem sie die
Funktion der Pili, kleinen haarähnlichen Fortsätze,
einschränken. Dadurch, dass sich die Keime nicht mehr »festhalten« können,
werden sie schneller fortgeschwemmt und können kein Unheil anrichten.
Mit Galliumionen nutzen Forscher das Prinzip
der Täuschung. Die Galliumionen werden von der
Biochemie des Bakteriums (den »Siderophoren«) mit Eisenionen verwechselt. Die Siderophoren
können kein Eisen mehr in die Bakterien schaufeln, welches sie aber brauchten,
um zu wachsen und Energie zu gewinnen. Die Bakterien werden dadurch lahmgelegt.
Ins Apothekenregal haben es diese Wirkstoffe bislang nicht geschafft,
ebenso wenig wie die Nanoschwämmchen und andere Pathoblocker. Noch steht etwa der Beweis aus, dass sie auch
Menschen helfen können.
Es müsse außerdem geklärt werden, ob sie auch bei einer ausgebrochenen
Infektion wirken, sagt Mark Brönstrup vom
Helmholtz-Zentrum für Infektionsforschung in Braunschweig. Zudem könne die Spezifität vieler Pathoblocker
-also dass sie genau auf eine Erregergattung zugeschnitten sind- eine Schwäche
darstellen: "Um den richtigen Wirkstoff einsetzen zu können, muss der Arzt
zunächst wissen, welche Bakterienart hinter der Infektion steckt. Das setzt
eine sehr genaue Diagnostik voraus, die Zeit kostet." Bei einer akuten
lebensbedrohlichen Infektion sei ein Breitbandantibiotikum unter Umständen die
sicherere Alternative.
Dem Körper beim Helfen helfen
Der Biologe Jörg Hacker, Präsident der Deutschen Akademie der
Naturforscher Leopoldina, schreibt den Pathoblockern aber durchaus Zukunftspotenzial zu: "Der
Ansatz ist vielversprechend, und ich halte es für wichtig, ihn
weiterzuverfolgen." Große Hoffnung setzt er zudem in sogenannte
wirtsbasierte Therapien, die ebenfalls nicht direkt den Krankheitserreger
bekämpfen, sondern stattdessen das Immunsystem des Erkrankten aktivieren. Das
bekannteste Beispiel ist die klassische Impfung. Eine neuere Form der
Immuntherapie, die auch gegen resistente Erreger helfen könnte, beschrieb
kürzlich eine Forschergruppe um den Immunologen Wilhelm Schwaeble
von der Universität Leicester. Sie kreierte mit gentechnischen Mitteln eine
besonders aktive Variante des natürlichen Bluteiweißes Properdin,
das dafür zuständig ist, unsere körpereigene Abwehr in Gang zu setzen. Um den
Schutzeffekt des Eiweißes zu verstärken, erschuf das Forscherteam im Labor eine
aktivere Version. Bei Labormäusen zeigte es eine sehr gute Wirkung gegen
tödliche Meningokokkenkeime.
"Eine septische Meningokokkeninfektion
führt beim Menschen unbehandelt zu einer Sterblichkeit von bis zu 40%. Und
selbst nach optimaler Behandlung mit Antibiotika liegt die Sterblichkeitsrate
von Patienten mit septischem Schock bei zehn Prozent, also noch inakzeptabel
hoch", sagt Schwaeble. Denn Antibiotika töten
zwar die Bakterien ab, diese setzen dabei jedoch ihre giftigen Bestandteile
frei. "Der größte Vorteil unserer Therapie ist, dass im Zuge der durch das
künstlich hergestellte Properdin aktivierten,
natürlichen Immunantwort auch die giftigen Keimteilchen unschädlich gemacht
werden", sagt Schwaeble. Er und sein Team planen
weitere Experimente mit anderen Krankheitserregern, auch mit MRSA. "Da Properdin ganz anders wirkt als Antibiotika, sehe ich
keinen Grund, warum es nicht auch gegen resistente Erreger wirken sollte",
sagt er. Aber erst in vier bis fünf Jahren sind Tests am Menschen geplant.
Es ist zwar möglich, dass Properdin sich als
unwirksam entpuppt oder unerwünschte Wirkungen zeigt. Die Gefahr besteht bei
den meisten neuartigen Behandlungsmethoden. Dennoch könnten die neuen Ideen
eine Grundlage für zukünftige Therapien liefern. "Wir werden vielleicht
nie ganz ohne Antibiotika auskommen, und wir brauchen dringend neue antibiotische Stoffklassen – aber es ist auch an der Zeit,
dass die Forschung ausgetretene Pfade verlässt", sagt Leopoldina-Präsident
Jörg Hacker. Und dann kann vielleicht auch Menschen wie Gerda Jäker geholfen werden.
[Jacqueline Smith]
The aim of this review has been realised, in that, by utilising
homeopathic methodology, the genus epidemicus has
been identified and subsequently six main remedies considered as being appropriate
for treatment of the documented stages of the disease process from inflammation
through to necrosis in susceptible individuals. The information reviewed
concerns both the accepted theory and practice of treatment of the disease
process in N.F. which can result in states of inflammation, suppuration,
gangrene or finally necrosis as a consequence of puncture wounds (caused by
drug injection), repeated over time or infected by an exogenous pathogen in
those with a compromised immune system (C.I.S.), and the theory and practice in
homoeopathy for treatment of similar states, with similar causes. This paper
supports the assertion that homoeopathic treatment is a viable alternative when
antibiotics are proving ineffective.
AIM
To identify a group of appropriate homoeopathic medicines, which can
potentially be used in threatening or actual suppuration in abscesses and
necrosis of same or other local sites, in susceptible individuals. In this
review I consider particularly those of homeless status who are also
intravenous drug users (especially of heroin).
To discuss risk factors which
predispose some individuals to a lowered immune system who are therefore more
susceptible to developing or contracting Necrotising Fasciitis (N.F.)
To examine details of
documented and possible bacteria involved in the process of suppuration leading
to necrosis.
To consider relevant
homoeopathic philosophy in relation to susceptibility, maintaining causes, and
predisposition.
To outline the disease process
involved which may lead in some individuals, to developing N.F.
To present a resume of
individualised homoeopathic remedies potentially suitable for use in all stages
of the disease process outlined in Objective Four.
Background
In June 2000, 22 drug users in Scotland and 21 between Dublin and
Manchester, died after contracting (or developing) Necrotising Fasciitis, and
again in July 2001 eight individuals were affected, either fatally or requiring
surgical debridement +/o.partial amputation. These
cases were thought to be the result of using contaminated heroin for injecting
in cases of drug addiction. The condition itself is described as “… a rapidly
progressive soft-tissue infection that involves superficial and deep fascia
leading to thrombosis of cutaneous vessels and
gangrene of underlying tissues.” It was
first documented by Fournier in 1883 (4), and Meleney
isolated a particular bacteria as a causative factor in 1924. The term
‘necrotising fasciitis’ was ascribed to Wilson, who, in 1952, noted that an
“essential component” of gangrene with a specific bacteria, involved the deep
fascia. The condition can occur in any anatomical location, usually at a
distance from any trauma but also at affected sites. Other names that it is
known by e.g. Fournier’s Gangrene (genital), Meleney’s
Ulcer or Hospital Gangrene etc., often indicate either anatomical sites or
places where infection was contracted or developed. Conventional therapy
involves antimicrobial treatment with e.g. Penicillin, aminoglycoside,
metronidazole etc. and Hyperbaric Oxygen Therapy
(HBO) and surgical excision, including debridement and amputation when
considered necessary.
Necrotizing fasciitis left leg
There are several factors, which are conventionally regarded as leading
to possible susceptibility in contracting or developing N.F. The greatest of
these is that of having a ‘compromised’ immune system, which is noted in
conditions such as; Diabetes Mellitus, malignancy, renal impairment and trauma.
In this discussion, which is intent on reviewing the specific factors in
relation to the circumstances of intravenous drug users who may be homeless,
two of the above noted conditions are worthy of further exploration. In the
first instance, similar to Diabetes Mellitus II, where a state of ketosis may
develop due to the inability of the body to utilise carbohydrates and glucose,
it is worth pointing out that it is also possible for ketosis to develop in
states of starvation or eating disorders. The result being, that fats and
proteins become the primary energy sources, which may produce ketones in the blood, and thereby lead to ketoacidosis. In the report of a survey carried out in 1999
by the Office of National Statistics titled, ‘Health and Well Being of Homeless
People in Glasgow’ published in June 2000,
“19% of respondents had eaten only once in the day prior to interview
and 5% had not consumed any food at all. Fifteen per cent of respondents did
not consume any hot food (excluding drinks) in the day prior to interview.”
It would seem probable that in such circumstances, it would be possible
for heroin addicts who are also of homeless status to be at similar risk to
developing a condition akin to ketoacidosis, which
may also result in renal damage.
In addition, it is well known that nutritional deficiencies play a
decisive role in the prevalence and severity of microbial diseases in under
privileged people. The rate of wound healing is also markedly influenced by
dietary factors especially in deficiencies of some vitamins including Vitamins
C, E, K, B6 and Minerals such as Calcium and Iron.
The citing of ‘trauma’, as a further risk factor is particularly apt in
the present examination of the incidence of N.F. in intravenous drug users.
‘Trauma’, here being defined as: “…any injury caused by a mechanical or
physical agent.”
Heroin addiction most often requires the use of intravenous means
whereby the subjects repeatedly inject the drug, causing puncture wounds, often
several times daily for, perhaps, a duration of some years, with little or any
use of disinfecting measures. Thus creating a higher than usual risk of
infection at multiple sites, most often on arms and legs but the groin area is
also used amongst others, as more accessible veins become unusable.
In the outbreaks of N.F. documented here, this is all the more relevant,
for it has been discovered that all the cases had a significant factor, i.e.
the injection has been made directly into muscle tissue or accidentally into
other tissues when a vein has been missed. This assertion also brings to bear
the immune inhibiting effects of drugs themselves as a risk factor to infection
which include non-steroidal inflammatory preparations such as aspirin,
ibuprofen, naproxen etc. that inhibit the inflammatory mechanism that makes
tissue repair possible. Steroid use is particularly implicated, possibly due to
the fact that cortisone interferes with the production of antibodies under
certain conditions.
This immunologic inhibition cannot account entirely for the infection
enhancing effect. In addition to interfering with antibody production,
cortisone influences many other physiologic processes, some of which may affect
directly or indirectly the response of the body to infection. Interference with
the inflammatory response and with the activity of the reticulo-endothelial
system, disturbance of the intermediary metabolism, and activation of proteo-lyctic enzymes are but a few of the effects of
cortisone that might be important in this regard.
The habitual use of heroin, (= diacetyl-morphine,
a semi- synthetic compound derived from morphine and stronger than the natural
drug), which has its effects principally on the (CNS) and also affects some
peripheral organs such as the alimentary tract and the respiratory system, is a
definite factor in compromising the immune system. Morphine usually neither
eliminates the psychological perception of pain nor blocks the sensation.
Although there are exceptions, the person knows that pain continues, but he or
she is not disturbed by it. The associated fear and tension subside so that the
pain becomes bearable. These reactions signify the effects on the CNS but the
opiates may also change the activity of peripheral nerves that conduct messages
to and from the brain.
The enkephalins involved are found in neurons
in the spinal cord and portions of the hind and mid-brain which transmit pain
and related sensory signals (for example, heat and cold), and in parts
of the mid-brain associated with movement, mood and behaviour. The enkephalins are also found outside the central nervous
system in the neurons of the periphery and the gut. These effects have
relevance in two areas in connection with this investigation: the fact that the
addict despite feeling hunger is able to ignore these feelings. This can result
in the production of acids in the gut which having no food to breakdown will
tend to become destructive to the alimentary tract itself. The other danger is
that by being able to ignore sensations of heat, pain and even fear for health,
any inflammation, abscess formation or numbness can continue unabated.
In the past, several types of bacteria have been identified as being
involved in the presentation of N.F. On this basis, two types of N.F. had been
labelled, i.e. i) Polymicrobial,
involving a number of organisms in various combinations and ii) Pure group A
Streptococcal, which is said to be haemolytic, (rupture of RBC membrane). In
direct relation to the cited outbreaks, Clostridiun Novyi Type A among others, was isolated from 18 of the
people who developed N.F. in June 2000. Some of these bacteria are known as
being indigenous (ie. present in a healthy state) to
the human body, e.g. Bacteroides, Staphylocci,
Streptococci, Pseudomonas aeruginosa, Clostridium
etc.
Two aspects are known to be observable concerning these micro-biota:
That most micro-organisms
commonly harboured by the body in a state of health are capable of exerting a
wide range of pathological effects under special conditions and,
Many of the micro-organisms
classified as pathogens, indeed probably all of them, often persist in vivo
without causing overt disease.
As has been previously noted, nutritional deficiencies, exposure to
toxic agents, and certain kinds of physiological stress are among the many
causes of disturbances associated with disease processes caused by indigenous microbiota.
In other words, some form of pathological or at least abnormal state
must exist before indigenous bacteria can multiply to such an extent that it
causes deleterious effects. George Bernard Shaw echoed Pasteur who suggested
that a physiological disturbance might in certain cases be the primary cause of
the infectious process rather than its consequence, when he said: “The
characteristic microbe of a disease might be a symptom instead of a cause.”
Early in the investigations of 2000, Dr Laurence Gruer,
Consultant to the Greater Glasgow Health Board commented that:
“It is quite possible that no single cause for the illnesses will be
identified. Many injectors in the affected areas of Glasgow have said that
their recent supply of heroin has required unusually large amounts of citric
acid to be added before it can be dissolved for injecting. A variety of
different bacteria normally found on the skin have been isolated from tissue or
blood from several patients.
It is likely that injection of the unusually strong heroin and acid
mixture can cause severe damage to muscle and other tissue. This may then
create the conditions for harmless bacteria present in heroin or carried on the
needle from the skin to cause serious infection.”
Clostridium Novyi, Type A, was isolated in
some, though not all, recent or current cases of N.F. at the time and described
as an “…’anaerobic’ bacteria-that is, they only grow in the absence of oxygen
(dead tissue). Some Clostridium can not only cause severe infection in damaged
tissue but can also produce very powerful toxins. They can also exist in for
years in dust or soil as dormant spores, only becoming activated when the
conditions are right.” But it was only previously been known to cause serious
infection in domestic animals; very rarely in humans and is commonly found in
soil and animal faeces. Other types of Clostridium have been located in
intestinal flora of the human where it is non-spore forming.
It is therefore a matter of postulating whether the Clostridium isolated
in the cases cited, is the actual cause originating in contaminated heroin
supplies and therefore exogenous. In classical infections of exogenous origin,
the determining etiological event of the disease is said to be exposure to the
infective micro-organism. This was yet to be made clear in the present
situation. The author has been unable to locate documentation on this
particular strain of Clostridium (ie. Novyi) in standard textbooks on microbiology and this raises
two questions:
In which conditions, if any,
has it been previously been isolated?
Or, is it a possible new
mutation arising from this particular combination of factors met in this
incidence of drug injectors?
In indigenous microbial disease, the immediate cause is the
environmental factors that upset the biological equilibrium normally existing
between the host and the microbial agents.The
documented factors common to many (but not all) of the affected were:
They are all Heroin Injectors,
whose supply source may or may not have been the same.
Many, if not all, used more
Citric Acid than usual to dissolve the drug for injection.
The subjects all injected into
muscle or tissue other than a vein.
If the source of supplied heroin was the same and all users of this
supply increased the quantity of Citric Acid – plus the involvement of the
injection into muscle and other connective tissue, (which is not particularly
uncommon in heroin addicts), not all heroin injectors likely to have used this
batch of the drug under these circumstances, have succumbed to either infection
or development of N.F. It would have to be considered somewhat as a result of
this combination of factors or it would suggest another unidentified
predisposing factor. Dr. Jai Lingappa, Epidemic
Investigation Officer at the Centers for Disease
Control in Atlanta, commented that:
“A lot more work still needs to be done to clarify how exactly the
Clostridium Novyi is contributing to the
illness……..We also want to learn more about why these people became sick and
others didn’t.”
Miasmen.:
Even from the viewpoint of conventional medicine, a person in robust
health may easily resist exposure to even the most virulent microorganisms. The
degree of resistance can change from hour to hour and day to day depending
upon exhaustion, starvation, cold, overwork, emotional stress, etc. It
has been stated clearly in a standard textbook on microbiology used in all
universities and medical schools in the U.S., that the susceptibility factor is
so significant that it is virtually impossible to decide the infective dose of
a specific microorganism. In the cited cases of those developing N.F., this
study has identified at least some of the major factors related to increased
susceptibility to developing a seriously life threatening infectious disease
and this is further explained in Homoeopathic philosophy by considering not
just the ‘compromised’ immune system but by also considering the effects on the
Defence Mechanism of the human organism. This defence mechanism is known in
homeopathy as the Vital Force and is considered in terms of electro-dynamic
vibrations, which involves a great degree of complexity.
“The vital force level of the human organism is considered the dynamic
plane, affecting all levels of the being at once with varying degrees of
harmony and strength. It is a highly complex, fluid, flexible, and energetic
process, simultaneously responding to and affecting the surrounding
environment……The whole organism, and any component of it, can be strengthened
or weakened depending upon the degree of harmony, resonance, and force of the morbific or therapeutic influence applied to it.”
When the strength of a noxious trigger is stronger than the strength of
the vital force, the defence mechanism is called into play to counteract the
stimulus. If the vital force is so weakened by exciting and maintaining causes,
any powerful noxious trigger would alter the state of the entire organism
without adequate defence, and death would rapidly ensue. There is a latent
period before actual symptoms develop, during which the defence mechanism
begins
to adjust to the effect of the stimulus. In bacterial infections this
ranges from hours to days.
From this premise it should be clear that disease is a result of a morbific stimulus which resonates with the particular
susceptibility of the organism. This stimulus is known as the exciting cause
and may be a microorganism, a foreign chemical, an emotional shock, a
vaccination, etc.
Maintaining causes are those factors external to the organism which,
because they continue to affect the individual over a period of time, maintain
the individual in a weakened state eg. Lack of
nutrition, unsanitary or damp living conditions, drug addiction; conventional
drugs prescribed for long periods or repeated often in short periods of time
(also regarded as Iatrogenic miasms), repeated
emotional trauma, in short, many of the factors previously mentioned. But yet, the predisposition underlying much
of these areas of susceptibility is the Fundamental Cause.
“Useful to the physician in assisting him to cure, are the particulars
of the most probable exciting cause of the acute disease, as also (are) the
most significant points in the whole history of the chronic disease to enable
him to discover
its fundamental cause, which is generally due to a chronic miasm. In these investigations, the ascertainable physical
constitution of the patient, his moral and intellectual character, his
occupation, mode of living and habits, his social
and domestic relations, his age,… etc., are to be taken into
consideration.” (Para. 5, The Organon of Medicine,
Samuel Hahnemann, 5th & 6th Edition, B.Jain Pub.
Reprint 1992)
The theory of Chronic Miasms is complex and
involved and it is not within the scope of this review to give a full
explanation of such. (Please see Bibliography section for further study). In
summary, it is sufficient to say that a miasm
is a resulting stereotypical disease condition, sometimes heredotransmissable, which can be latent or active, acute
or chronic. Nevertheless, it is always the result of both a maintaining cause
(hence the lingering disposition) and an exopathic
exciting cause (the noxious trigger).
There is one miasmatic pattern, relevant to
this review that has been recognised for most of Homoeopathy’s history ie., the Luetic Miasm. This particular pattern is in essence one of
destruction and disintegration. There will often
be a predilection in the family history to similar patterns of
destructive illnesses, eg. Syphilis, alcoholism,
conditions where ulceration has taken place or a tendency to necrosis, etc.
When active and predominant in an individual, this pattern will taint and
distort expression at all levels, mental, emotional and physical. In the
individuals involved in the outbreaks of N.F. cited , the destructive pattern
is essentially seen in addictive habits concerning the use of heroin and often
several other substances. There exists a craving for acidic or spicy foods in
general, there is a metabolic tendency to acidity and they are often of a
temperament conducive to states of rage; that is when not suppressed by drugs.
The effects of this pattern whereby heroin addiction is a symptom result in
destruction not only of the immune system and particular bodily organs and
systems e.g. the heart and circulatory system, but as noted, affects the
intellectual faculties, the emotional responses and subsequent behaviour
destroys family and social contact.
With regard to the ‘contagious principle’, Hahnemann, (1755-1843,
founder of Homoeopathy), though not having the benefit of a microscope, put
forward an uncannily accurate explanation more than half a century ahead of
Robert Koch and others. He suggested in 1832 (Lesser Writings, p.758) that
cholera, for instance, was caused by “…an enormous …brood of excessively
minute, living creatures.”
He also regarded each epidemic (acute miasm)
as having features of its own (the genus epidemicus)
And since it is always the product of a single cause it will, in all individual
cases, be amenable to one and the same specific remedy, the epidemic’s simillimum.
The Disease or better Illness:
In this section, the disease process taken into account is that which
begins, for our purposes, from the available information on the circumstances
and states of individuals who were involved in cited presentations of actual or
threatening N.F.
They are individuals who are:
Intravenous Drug users i.e.,
heroin injectors;
Experience a chaotic
lifestyle, which often includes bouts of homelessness.
Deaths predominantly in
females.
In the first assertion, two factors are particularly important:
1a). Lowered Immune System due to chronic heroin use (poisoning);
1b). Bodily subjected to repeated trauma from puncture wounds.
In the second assertion, two factors are again considered of import:
2a). Immune system further compromised by chaotic lifestyle, especially
during times of homelessness, resulting in:
Reduced
intake of adequate food and nutrition.
Exposure to the elements.
2b). Less access to medical services when required, unless in an
emergency.
This information provides some clues to the degree of susceptibility at
the general level of health and the particular susceptibility at the physical
sites by repeated trauma and risk of infection.
DISEASE and DRUG ACTION in HOMOEOPATHIC CONGRUITY
Applied therapeutic science requires a coincident parallelism between
the symptom complexes of both the disease and the drug of choice on as many of
the first seven under-mentioned points of comparison as possible. Obvious
incongruity in any comparative aspect frequently amounts to symptom
dissimilarity in the case, allowing for the elimination of many otherwise
eligible remedies, facilitating the process of repertorisation.
1. Generic Similarity
Homoeopathicity of type of affliction; describes
the identity in the class of affections induced by both the natural disease of
the patient and the experimental disease of the drug to be used: eg. I) if the illness is febrile, the remedy must be pyrogenetic; ii) if the disease is an inflammation, the
drug of choice will be an irritant, etc.
Causal Similarity
Homoeopathicity of formative affectors;
means that the antecedent concomitants present when the disease arises will
substantially narrow the field of contenders among drugs to be used: eg. I) neuralgia induced by injury to a nerve is different
from one brought on by shingles and that again is also distinct from one that
comes on with gout.
Parallels in Symptom
Modalities
Homoeopathicity of modalities. Meteorological and
thermal influences, cosmic rhythms, mental factors, physical conditions
(including movements and rest), relation to food and drink, location,
laterality and time are circumstances that can contribute to making symptoms I)
better or ii) worse, iii) appear or iv) change.
Symptom Character Resemblance
Homoeopathicity in the quality of abnormal
sensations. All sensations have a distinct character: for instance, a gnawing
pain, a burning pain, a tearing pain etc. are distinctly different from each
other. The character of such sensations are to be alike in both the disease and
the drug action.
Constitutional Compatibility
This describes the aggregate of patients’ common features. It is used to
identify patients according to their temperament, appearance, certain
characteristics of behaviour and their variance from the normal, which should
be compatible with the corresponding remedy.
Synchronicity of Symptom
Evolution
Homoeopathicity of pharmocodynamic
devolution; meaning that various developmental aspects of the disease process
of the patient must synchronise with the developmental pathogenicity
inherent in the drug to be applied.
Concordance of Emotional
Symptoms
Homoeopathicity of disposition; matching emotional
and/ or the intellectual symptoms. Since mental and emotional symptoms are in
evidence well ahead of functional and morphological changes when disease
develops, they frequently provide very early indications for homoeopathic
treatment.
Matching of Three or More
Guiding Symptoms
Multiples of semiological homoeopathicity.
Reliance on the coincidence of three, but preferably more, striking symptoms,
evident in both the artificial illness of a drug as well as in the phenomena of
a disease, rests on the mathematical law of permutations. If three distinctive
symptoms of a case can be found to have been experimentally produced by a
medicine, there is already considerable likelihood of its acting on the same
parts and in the same manner.
Ranking
Many homoeopaths are guided by Robert Gibson Miller, who in 1910
proposed ranking the above points of comparison in the following order of
priority:
matching mental &
emotional symptoms;
correspondence between
modalities of time, season, motion, locality, sensation etc.
similarity of pronounced
cravings and aversions;
menstrual, or hormone-related,
changes in state in both the natural and the artificial diseases;
resemblance between the
particulars as well as the generals of both diseases, where only the peculiar,
unexpected, striking or unaccountable symptoms are of significance;
common symptoms, as featured
in standard non-homoeopathic disease classifications.
The Simillimum is the medicine, which in its
manifestations most clearly reflects the total symptom picture of the
individual’s diseased state, which will certainly cure that patient, if the
patient’s condition is within reversible limits. (28) In relation to the
symptoms available from the documentation in the author’s possession, which
have little or no individuality, it is less likely that the most accurate simillimum will be found. But as will be explained, it is
not always the best remedy to prescribe even if it were possible (ie, by taking information from those who are displaying
symptoms associated with the recent outbreak or who are thought to be at
greatest risk.)
Contra-indication Against Administering Simillimum
In a patient, whose disease is terminal and which may be in its final
stages, namely where the life force is hopelessly overwhelmed by the forces of
disease, or in many emergencies, it is absolutely contra-indicated to prescribe
the individual’s simillimum, which would, in these
circumstances, only be able to produce an aggravation hastening death. In such
an instance functiotropic, organotropic
or pathotropic remedies ought to be the homoeopathic
drugs of choice, with the intention of inducing a measure of improvement for
the limited period remaining to the patient. Therefore, the remedies identified
by using predominantly common, general and particular symptoms which have no
modalities, will be sufficient when given at the appropriate phase in the
disease process and may reflect more the nature of the Genus Epidemicus rather than the simillimum
of the individual patient.
Finding the Genus epidemicus
Although, it is not as yet possible to find, or would in some cases be inappropriate
to utilise the simillimum, many of the above
mentioned principles will still be employed to find the remedy or remedies that
come closest to the picture of the genus epidemicus.
This means that, depending on at which stage of the disease process the remedy
is administered, there is a possibility of preventing the development of N.F.
or reducing the effects of infection before it reaches a life threatening degree.Symptoms will be taken from all general and
particular disease processes outlined above:
Repertorisation using Synthesis (R.H.S.) Edition
5.2 Edit. Dr. Frederick Shroyens
GENERALS:
Wounds:
1. Penetrating (Punctured) +. Stab wounds, Synth.
Pg. 1720; APIS, Arn, Carb-v,
Cic, Hep, HYPER, lach, LED,
Nit-ac, sil, sulph.
2. Bluish + Black, Synth. Pg. 1719; Apis,
China, LACH.
3. Suppurating, Synth. Pg 1720; Arn, asaf, Bell, Calc, Calen, Cham,Chin, Hep Lach, Led, Merc, Sil, Sulph
4. Dissecting, Synth. Pg. 1719; Anthraci,
Apis, Ars, kreos, Lach, Led, Pyrog.
5. Gangrene of, Synth. Pg. 1719; Anthraci,
ARS, Bell, Calen, Carb-v,
China, LACH, sil,vip.
Inflammation:
6. Wounds, Synth. Pg. 1619; Arn,
hyper, lach, led, sulph.
7. Gangrenous, Synth. Pg. 1618; ARS, bapt,
Carb-v, hep, Iod, kreos, LACH, merc, Phos ,SIL
Abscesses:
8. To abort, Synth. Pg. 1547: Apis, arn, bell, bry, calc, calc-s, hep, merc.
9. Absorption of pus, Synth. Pg. 1547; Iod; LACH; Phos; Sil.
10. Gangrenous; Ars; asaf;
carb-v; chin; hep; kreos;
LACH; merc; nit-ac; phos; sil.
FEVER
Septic; Synth. Pg.
1487: ANTHRACI; Apis; ARN; ARS; BAPT; Bell;
BRY; Carb-v; LACH; Merc;
PHOS; PYROG; SULPH.
Zymotic;
Synth. Pg. 1490: Anthraci; apis; ARN; ARS; BAPT; Bell; BRY; carb-v;
hyos; ip; LACH; Merc; op; Phos; Puls; Pyrog; Sulph.
MIND
13. Morphinism:
Ars, bell, calc; cham; hyos, ip, lach,
merc, op; phos; puls.
Each remedy rated by the number of rubrics in which it appears and by
how prominent or characteristic it is in the remedy picture, ie. Those in
CAPITALS, are given 3 points; in Italics, are given 2 points; in plain type are
given 1 point.
REMEDIES (present in SIX or more Rubrics) + Points Rating / No. of Rubrics
|
|
|
Stage of Disease Process where appropriate to
use. |
|
|
|
|
28 / 12 |
*GENUS EPIDEMICUS- Rapid Onset Necrotising Fasciitis * |
|
|
|
|
|
16 / 7 |
Structural
Changes Necrosis – Life threatened.
*Suppuration/Dysfunction Struct. Ch. & Necrosis |
|
MERC. SOL. |
11 / 7 |
|
|
|
|
|
APIS
|
12 / 6 |
E. C. - PW: G. I. R Inflam. Sens. Dysf. /Supp Struct. Ch. *E. C – PW: G. I. R. Inflamm. Sens. Dysfunction |
|
|
|
|
12 / 6 |
|
|
|
|
11 / 6 |
Suppur. /Dysfunct. Structural Change (Gangrene)*E. C – PW: Suppur. / Dysfunct. Struct. Ch. Gangrene |
|
|
|
|
10 / 6 |
|
|
BELLADON. |
9 / 6 |
G. I. R Inflamm. Supp. /Dysf. Structural Change*E. C – PW: Pyrexia (toxic) Struct. Ch. Gangrene |
|
CARBO-VEG. |
9 / 6 |
|
|
|
||
|
KEY: E. C.
= Exciting CausePW: =
Puncture WoundsG. I. R. = General Inflammatory Response |
||
|
|
||
REMEDY
SCORE
Stage of Disease Process where
appropriate to use.
LACH. 28 / 12 *GENUS
EPIDEMICUS- Rapid Onset Necrotising Fasciitis *
ARS. 16 / 7 Structural Changes Necrosis – Life threatened.
*Suppuration/Dysfunction Struct. Ch. & Necrosis
MERC. 11 / 7
APIS.
12 / 6 E.
C. - PW: G. I. R Inflam. Sens.
Dysf. /Supp
Struct. Ch. *E. C – PW: G. I. R. Inflamm. Sens.
Dysfunction
ARN. 12 / 6
PHOS. 11 / 6 Suppur. /Dysfunct. Structural Change (Gangrene)*E. C – PW: Suppur. / Dysfunct. Struct.
Ch. Gangrene
SIL. 10 / 6
BELL. 9 / 6 G.
I. R Inflamm. Supp. /Dysf. Structural Change*E. C – PW: Pyrexia
(toxic) Struct. Ch. Gangrene
CARB-v. 9 / 6
KEY:
E. C. = Exciting CausePW:
= Puncture WoundsG. I. R. = General Inflammatory Response
MATERIA
MEDICA for GENUS EPIDEMICUS
LACHESIS
Poisoning
Symptoms: All the vipers are venomous; severe pain comes on at the site of a
bite, bloody serous discharge and ecchymoses in the
vicinity of the bite and thrombosis, followed, if not at once fatal, by local
inflammation and sloughing, and even gangrene.
Swelling
and black or purple discolouration of a limb may follow. Fever, with delirium and blood poisoning,
sets in, followed by suppuration, haemorrhage or gangrene. Death may follow a bite from the following
causes:
If a vein has been pierced, quickly from
thrombosis;
after some hours from heart failure, through
paralysis of the vasomotor centres;
after a few days from secondary bleeding;
later from septic infection of the necrotic
area around the bite.
Pharmacology:
The venom of Lachesis contains a full range of potent
enzymes, proteolytic, cytolytic,
neurotoxic and coagulant. One or more of these effects may
predominate. The blood is attacked
primarily, while, the nervous system is at first aroused and excited. The main affinities therefore are with the
blood, causing disintegration of red cells, lowered coagulability
after initial tendency to thrombosis, and impaired resistance to infection with
associated liability to gangrene and necrosis.
Also the CNS, with ensuing delerium, coma and
paralysis of vital centres. Also with
the cardiovascular system as evidenced by hypotension, cold sweats and
collapse.
Therapeutics:
The great blood-disintegrating (haemolytic) powers of Lachesis
are utilized in a number of febrile, septic, toxic and typhus-like conditions,
present in many named diseases, and in some forms called ‘malignant’ exanthems, where the body resistance has more or less
completely broken down. When this point
is attained the distinguishing or diagnostic features of the particular
diseases have largely disappeared.
Professor Teale: “Widely different bacteria
may produce very similar clinical features… when profound poisoning occurs,
instead of the poisoning becoming more, it becomes less characteristic, and
clinically is seen to be in the typhoid state. ”
Leading
Indications:
Severe cases where “blood-poisoning” is
marked: ‘low’ fevers, where blood-destruction or haemolysis is conspicuous,
conditions called typhus-like (typhoid), or septic after parturition or autopsy
wounds. Such conditions occur late in
many fevers.
Milder cases, where vascular erethism is conspicuous-palpitation, hot flushes,
sleeplessness. Such a state is frequent
at the menopause or after arrest of physiological discharges or the sudden
arrest of pathological discharges, and relieved by the restoration of them. Shock may cause such a state.
Though sensitive to either extremes of
temperature, cases requiring Lachesis are chiefly
noted for intolerance of hot weather, hot rooms, etc. (direct rays of the sun).
Local symptoms are frequently left-sided or
move from left to right.
Sleep is not easily wooed; when it comes it
is restless and the patient usually wakes worse in every respect, so that he
fears to go to sleep.
The mental state varies… Incoherence,
degenerating to muttering delirium in fevers, is characteristic.
Over-sensitiveness to surface contact
(touch), and to constrictions, or even to clothing which is not too tight
(neck, abdomen, etc. )
A bluish hue around wounds, ulcers,
etc. from blood pigment, or venous
stasis.
Difficulty of swallowing, especially fluids, regurgitation through the
nostrils.
Onset of discharges tends to relieve most
symptoms.
Craving for alcohol, even in teetotallers.
Bleeding in many parts, blood dark and
thin; ecchymoses.
The type of patient a thin, melancholy,
indolent person, changed physically and temperamentally by illness.
<:
Morning/after sleep/extremes of
temperature/constriction/contact/acids/alcohol/spring/summer/empty
swallowing/hot drinks/motion/stooping/lying/emotions/lying on left side
(palpitation);
>:
From onset of discharges;
Causation:
Injuries. Punctured wounds. Poisoned wounds. Vexation.
Anger. Jealousy. Alcohol.
Sun.
DD.
:
Ars. : Tendency to rapidly proceed to a condition
of malignancy, ie. , diseases assume a grave form, to
the destruction of tissue, to a general lowering of the vital forces, and
haemolysis, ending, if not checked, in death.
Another characteristic is prostration, a
prostration that is out of proportion to the severity of the complaint. The patient is exhausted after the slightest
exertion.
Nevertheless, they are extremely
restless. Restless with the pains, must
walk about, which helps. Also mental
restlessness, feels impelled to move and when too prostrate wants others to
move them from bed to bed or room to room.
Pains have a burning character where-ever
situated in the body and there is often a sensation of hot fluid coursing
through the veins.
Generally chilly, despite the burning
pains.
Periodicity is a feature of Arsenicum. It occurs
every other day, every fourth, seventh, or fourteenth day: the more chronic the
complaint the longer the cycle.
Putridity of discharges. This is an accompaniment of its ulcerations
whether internal or external, and of the tendency of its ulcerations to go on
to necrosis and its inflammations to become gangrenous.
Allied with this is Inflammed
and ulcerated parts bleed readily. Haemmorrhages occur from the lungs, bowels, kidneys and
uterus.
<:
midnight/after 3 h. /cold/lying with head low/exertion/after (cold) food and
drink;
>:
From warmth, movement;
Merc. : A feature of Mercurius
is very easy exhaustion after quite slight exertion. Tends to emaciation and paretic weakness,
associated with a liability to fainting attacks or sudden myocardial
failure.
Blood
dyscrasias occur, resulting in profound anaemia which
renders the subject liable to ready suppuration, characterised by sanious pus or necrotic ulceration.
Leading
Indications.
Cachexia,
anaemia, exhaustion, emaciation.
Salivation; stomatitis.
Increase and alteration of secretions,
which become thin and excoriate.
Ulceration of skin and mucous membranes.
Perspirations which do not relieve and are
foul-smelling.
Thirst, with moisture of mouth and tongue.
Aggravation of all symptoms at night and
from warmth of the bed.
Moist eczema and intetrigo.
Nocturnal bone pains.
Low-grade suppurations, which are acrid and
blood-stained.
Tremors of course character that tend to
become convulsive.
Green, bloody or mucous stools with tenesmus, “a cannot get done feeling. ”
Foul body smell.
Mercurial symptoms occurring in syphilis.
Catarrhs of mucous membranes, with increased
mucous.
<:
at night/heat & cold/warmth of bed/draughts/bending forwards/after
eating/lying on right side/touch & pressure/motion & exertion/sweet
food/lamplight & firelight;
>:
rest/weeping/coitus;
Apis. : In addition to haemolysis, coagulation of
fibrinogen and increased permeability of capillaries, there is also a lowering
of surface tension and membranes potential, which results in reduction of
osmotic pressure and facilitates diffusion of fluids, leading to oedema and
effusion. (38)
Leading
Indications:
Aggravation from heat in any form.
Over-sensitiveness: of skin, of mind, of
organs.
Sadness, indifference, suspicion, jealousy.
Foolish or childish behaviour.
Stinging, burning pains, with rapid change
of site.
Violence and rapidity of complaints.
Right-sided; symptoms go from right to
left.
Absence of thirst where it is expected, ie. , during heat, and also generally.
Tight, constrictive sensations: in throat,
larynx, chest, abdomen.
Inflammation and oedema: of skin, mucous
membranes, serous membranes, synovial membranes, subcutaneous tissues.
Urticaria and
erysipelas.
Cerebral affections, especially in
children; meningitis, cri cerebral.
Morning diarrhoea.
Prostration; faintness.
<:
3 h.
(chills)/morning/evening/night/(radiant) heat/close rooms/touch &
pressure/lying down/getting wet;
>:
cold/cold washing/expectoration/sitting/changing position;
Arn. : Cause: any injury, however remote seems to
have caused the present trouble. After
traumatic injuries, overuse of any organ, strains. Arnica is disposed to cerebral
congestion. It acts best in plethora, in
debilitation with impoverished blood, cardiac dropsy with dyspnoea. A muscular tonic. Traumatism of grief, or remorse. Influenza.
Limbs and body ache as if beaten; joints as if sprained. Bed feels too hard. Sore, lame, bruised feeling.
Marked
effect on the blood. Affects the venous
system inducing stasis. Thrombosis. Haematocele.
Ecchymoses and haemorrhages. Relaxed blood vessels, black and blue
spots. Tendency to haemorrhage and
low-fever states. Tendency to tissue
degeneration, septic conditions, abscesses that do not mature. (41)
If
the malady advances more definite stupor develops, and though when roused the
patient begins to answer a question correctly, he lapses in the middle of a
sentence into muttering delerium or
unconsciousness. When a patient has
arrived at this mental state he is well on in a typhus, enteric, malignant
malaria, yellow fever, or sepsis (surgical, peurperal
or other). The concomitants in the shape
of muttering delerium, fever, rapid, weak pulse,
dusky skin, possibly with ecchymoses, or congestive
patches, dry tongue, sordes etc. some or all of these will now be
present. (42). Prophylactic of pus infection. (Shroyens,
Synthesis, Edit. 5. 2. , Pg. 1790)
<:
Walking/going upstairs/movement/spinal pain/wrist pain/various pains <
inspiration;
>:
Movement. (Sore feeling from lying on
one part, but the relief is only temporary);
Phos. : Therapeutics: In typhoid-like conditions
Phosphorus is recognisable by:
Abdomen
distension; sore, very sensitive to touch.
Stools offensive, bloody, involuntary.
The anus appears to remain open.
Worse lying on left side: better right.
Burning in stomach: burning thirst for cold water. Desire for ice cream.
Fear
alone; in dark; of thunder. Suspicious.
(44)
Sil. : Skin: Lymphatic swellings and abscesses,
even with fistulous ulcers. -Engorgement, induration
and suppuration of glands. -Abscesses which do not break, but burrow under the
skin; exanthemata in general which corrode and spread. Ulcers in general; wherever pus is discharged
from any part of the body; ulcers burning, scabby; indolent; when circumscribed
with redness; very high, hard ulcers; with proud flesh; with corroding pus;
smell very offensive. Inflammation,
softening(swelling), and ulceration of bones.
Mild and malignant suppurations, esp.
in membranous parts. Small wounds
heal with difficulty, and suppurate profusely.
Mental & Emotional: weak, nervous, easily irritated, faint-hearted;
yielding, giving up disposition, “grit all gone. ”
<:
cold or draft/motion/open air/at new moon;
>:
warm room/wrapping up head/magnetism and electricity;
Bell.
: Leading Indications
Congestions and inflammations of a violent
and intense character.
Pains and symptoms come and go suddenly and
are violent.
Tendency to delirium of an active and
violent kind: hallucinations, fears of imaginary things with desire to escape.
Tendency to twitchings,
jerkings and convulsions.
Burning fever and rapid pulse, which is
strong and bounding; early stages of inflammations.
Dryness and heat of the skin and mucous
membranes.
Hypersensitivity to all impressions,
drafts, noises, pressure etc.
Great thirst not relieved by drinking.
< in the afternoon (15 h. ) and till
after midnight.
Predominance of affections on the right
side.
Symptoms are worse in the horizontal
position (especially the head).
Tendency to rapid formation of pus in
external inflammations.
Carb-v. : Charcoal has the property of absorbing
gases in its intestines, and thus ordinarily contains quantities of oxygen
which, when the charcoal is brought into contact with decomposing organic
matter, is released, and oxidises the putrefying mass, while at the same time
the charcoal adsorbs the gases that are formed by the oxidising process. It has no direct action on the microbes of
putrefaction, but favours the development of the aerobic organism at the
expense of the anaerobic.
Leading
Indications:
Desire to be fanned rapidly in stomach and
respiratory complaints.
Burning internally, cold externally;
burning characterizes Carbo-v.
Surface cold; dusky blue nails; dilated
capillaries and veins, cold sweat.
Numbness of parts lain on.
Haemorrhages, passive oozing of dark thin
blood.
States of collapse, surgical shock.
Septic conditions, putrid discharges.
Conditions where there is a lack of
reaction.
Low states of vitality with venous
engorgement.
Fever: tertian type, beginning 9 – 10
h. Thirst in cold stage, none in hot.
<:
morning on waking/evening/hot, damp air/warmth/brandy &
wine/butter/pork/rich food/abuse of quinine and mercury;
>:
eructations/warm covering/being fanned;
Vorwort/Suchen. Zeichen/Abkürzungen . Impressum.